3
What is a Theory?
Theories are simply an explanation of something and can be valuable tools for understanding human behavior. In fact, developmental theories offer explanations about how we develop, why we change over time and the kinds of influences that impact development. Theory is usually the first step of conducting research. Theories help guide and interpret research findings by providing researchers with help putting together various research findings. Think of theories as a story that is used to both explain behaviors and to guide research. Each time a researcher conducts an experiment to test the validity of a theory another page is being added to the story. The instructions can help one piece together smaller parts more easily than if trial and error are used.
Historical Theories of Development
Today, children are widely seen as vulnerable individuals who need protection and care. Child labor is considered unacceptable, and society generally believes that children should be nurtured. However, this view has changed over time. Historically, children were viewed as “little adults”—they wore miniature versions of adult clothing and were expected to take on adult responsibilities. Their developing bodies and limited strength were not seen as reasons for extra care but rather as flaws. This perspective began to shift in the 18th century, as people started to recognize childhood as a distinct and important stage of development.
John Locke (1632-1704) [1]
John Locke, a British philosopher, refuted the idea of innate knowledge and instead proposed that children are largely shaped by their social environments, especially their education as adults teach them important knowledge. He believed that through education a child learns socialization, or what is needed to be an appropriate member of society. Locke advocated thinking of a child’s mind as a tabula rasa or blank slate, and whatever comes into the child’s mind comes from the environment. Locke emphasized that the environment is especially powerful in the child’s early life because he considered the mind the most pliable then. Locke indicated that the environment exerts its effects through associations between thoughts and feelings, behavioral repetition, imitation, and rewards and punishments (Crain, 2005). Locke’s ideas laid the groundwork for the behavioral perspective and subsequent learning theories of Pavlov, Skinner and Bandura.
Jean-Jacques Rousseau (1712-1778) [2]
Like Locke, Rousseau also believed that children were not just little adults. However, he did not believe they were blank slates, but instead developed according to a natural plan which unfolded in different stages (Crain, 2005). He did not believe in teaching them the correct way to think but believed children should be allowed to think by themselves according to their own ways and an inner, biological timetable. This focus on biological maturation resulted in Rousseau being considered the father of developmental psychology. Followers of Rousseau’s developmental perspective include Gesell, Montessori, and Piaget.
Contemporary Theories of Development
Psychoanalytic Theories
Sigmund Freud (1856-1939) and Psychoanalytic Theory [3]
 While sometimes controversial, Freud has been a very influential figure in the area of development; his view of development and psychopathology dominated the field of psychiatry until the growth of behaviorism in the 1950s. His assumptions that personality forms during the first few years of life and that the ways in which parents or other caregivers interact with children have a long-lasting impact on children’s emotional states have guided parents, educators, clinicians, and policy-makers for many years. We have only recently begun to recognize that early childhood experiences do not always result in certain personality traits or emotional states. There is a growing body of literature addressing resiliency in children who come from harsh backgrounds and yet develop without damaging emotional scars (O’Grady and Metz, 1987). Freud has stimulated an enormous amount of research and generated many ideas. Agreeing with Freud’s theory in its entirety is hardly necessary for appreciating the contribution he has made to the field of development.
While sometimes controversial, Freud has been a very influential figure in the area of development; his view of development and psychopathology dominated the field of psychiatry until the growth of behaviorism in the 1950s. His assumptions that personality forms during the first few years of life and that the ways in which parents or other caregivers interact with children have a long-lasting impact on children’s emotional states have guided parents, educators, clinicians, and policy-makers for many years. We have only recently begun to recognize that early childhood experiences do not always result in certain personality traits or emotional states. There is a growing body of literature addressing resiliency in children who come from harsh backgrounds and yet develop without damaging emotional scars (O’Grady and Metz, 1987). Freud has stimulated an enormous amount of research and generated many ideas. Agreeing with Freud’s theory in its entirety is hardly necessary for appreciating the contribution he has made to the field of development.
Freud’s Theory of the Mind
Freud believed that most of our mental processes, motivations and desires are outside of our awareness. Our consciousness, that of which we are aware, represents only the tip of the iceberg that comprises our mental state. The preconscious represents that which can easily be called into the conscious mind. During development, our motivations and desires are gradually pushed into the unconscious because raw desires are often unacceptable in society.
Freud’s Theory of the Self
As adults, our personality or self consists of three main parts: the id, the ego and the superego. The id is the part of the self with which we are born. It consists of the biologically driven self and includes our instincts and drives. It is the part of us that wants immediate gratification. Later in life, it comes to house our deepest, often unacceptable desires such as sex and aggression. It operates under the pleasure principle which means that the criteria for determining whether something is good or bad is whether it feels good or bad. An infant is all id. The ego is the part of the self that develops as we learn that there are limits on what is acceptable to do and that often, we must wait to have our needs satisfied. This part of the self is realistic and reasonable. It knows how to make compromises. It operates under the reality principle or the recognition that sometimes need gratification must be postponed for practical reasons. It acts as a mediator between the id and the superego and is viewed as the healthiest part of the self.[4]
The superego’s function is to control the id’s impulses, especially those which society forbids, such as sex and aggression. It also has the function of persuading the ego to turn to moralistic goals rather than simply realistic ones and to strive for perfection.
The superego consists of two systems: The conscience and the ideal self. The conscience can punish the ego through causing feelings of guilt. For example, if the ego gives in to the id’s demands, the superego may make the person feel bad through guilt.
The ideal self (or ego-ideal) is an imaginary picture of how you ought to be, and represents career aspirations, how to treat other people, and how to behave as a member of society.
Behavior which falls short of the ideal self may be punished by the superego through guilt. The super-ego can also reward us through the ideal self when we behave ‘properly’ by making us feel proud. If a person’s ideal self is too high a standard, then whatever the person does will represent failure. The ideal self and conscience are largely determined in childhood from parental values and how you were brought up.[5]
Freud’s Levels of Consciousness in Relation to the Id, Ego, and Superego
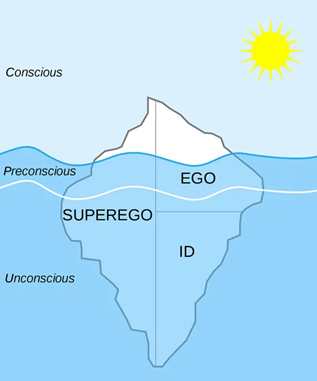
Freud’s description of personality shows that the ego operates primarily at the conscious level, but also operates somewhat at both the preconscious and unconscious level as does the superego. However, the superego operates mostly at the unconscious level whereas the id totally functions at the unconscious level. [6]
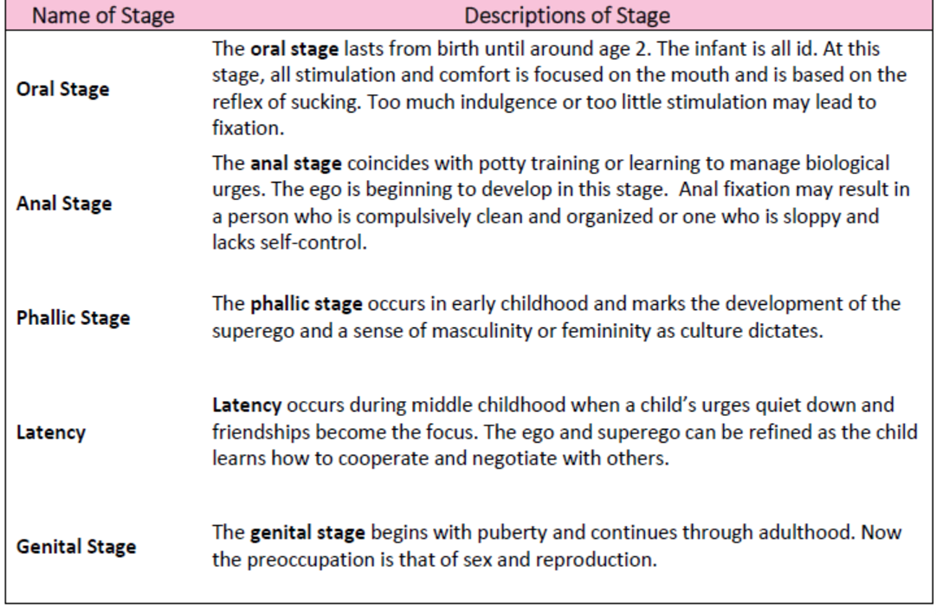
Psychosexual Stages
Freud’s psychosexual stages of development are presented in the table below. At any of these stages, the child might become “stuck” or fixated if a caregiver either overly indulges or neglects the child’s needs. A fixated adult will continue to try and resolve this later in life. Examples of fixation are given after the presentation of each stage.
Freud’s Psychosexual Stages
Strengths and Weaknesses of Freud’s Theory
Freud’s theory has been heavily criticized for several reasons. One is that it is very difficult to test scientifically. How can parenting in infancy be traced to personality in adulthood? Are there other variables that might better explain development? The theory is also considered to be sexist in suggesting that women who do not accept an inferior position in society are somehow psychologically flawed. Freud focuses on the darker side of human nature and suggests that much of what determines our actions is unknown to us. So why do we study Freud? As mentioned above, despite the criticisms, Freud’s assumptions about the importance of early childhood experiences in shaping our psychological selves have found their way into child development, education, and parenting practices. Freud’s theory has heuristic value in providing a framework from which elaborate and modify subsequent theories of development. Many later theories, particularly behaviorism and humanism, were challenges to Freud’s views.
Erik Erikson (1902-1994) and Psychosocial Theory[7]

Erikson suggested that our relationships and society’s expectations motivate much of our behavior in his theory of psychosocial development. Erikson was a student of Freud’s but emphasized the importance of the ego, or conscious thought, in determining our actions. In other words, he believed that we are not driven by unconscious urges. We know what motivates us and we consciously think about how to achieve our goals. He is considered the father of developmental psychology because his model gives us a guideline for the entire life span and suggests certain primary psychological and social concerns throughout life.
Erikson expanded on his Freud’s by emphasizing the importance of culture in parenting practices and motivations and adding three stages of adult development (Erikson, 1950; 1968).
He believed that we are aware of what motivates us throughout life and the ego has greater importance in guiding our actions than does the id. We make conscious choices in life and these choices focus on meeting certain social and cultural needs rather than purely biological ones. Humans are motivated, for instance, by the need to feel that the world is a trustworthy place, that we are capable individuals, that we can make a contribution to society, and that we have lived a meaningful life. These are all psychosocial problems.
Erikson divided the lifespan into eight stages. In each stage, we have a major psychosocial task to accomplish or crisis to overcome. Erikson believed that our personality continues to take shape throughout our lifespan as we face these challenges in living. Here is a brief overview of the eight stages:
Erik Erikson’s Psychosocial Theory
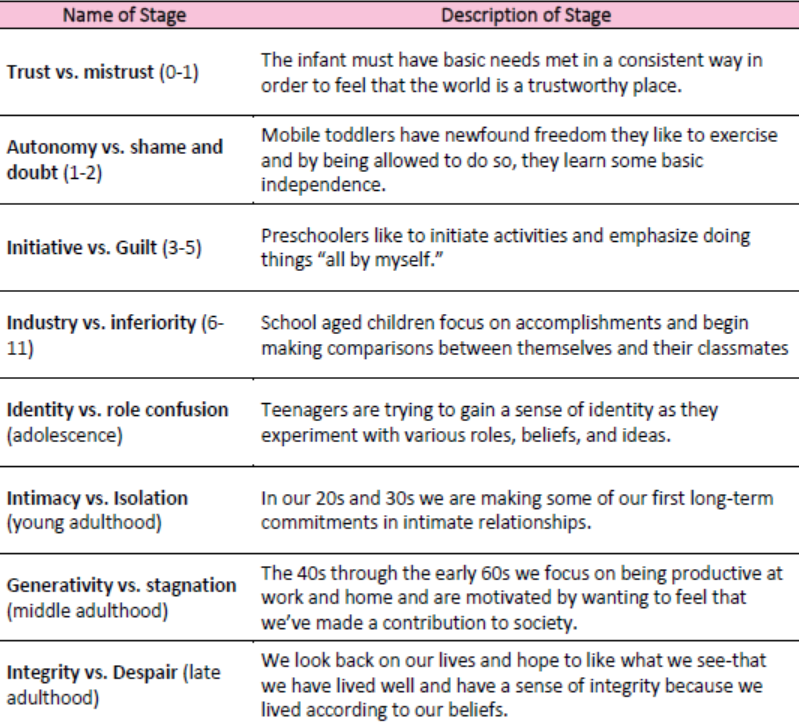
These eight stages form a foundation for discussions on emotional and social development during the life span. Keep in mind, however, that these stages or “crises” can occur more than once. For instance, a person may struggle with a lack of trust beyond infancy under certain circumstances. Erikson’s theory has been criticized for focusing so heavily on stages and assuming that the completion of one stage is prerequisite for the next crisis of development. His theory also focuses on the social expectations that are found in certain cultures, but not in all. For instance, the idea that adolescence is a time of searching for identity might translate well in the middle-class culture of the United States, but not as well in cultures where the transition into adulthood coincides with puberty through rites of passage and where adult roles offer fewer choices.
Behaviorist
While Freud and Erikson looked at what was going on in the mind, behaviorists rejected any reference to mind and viewed overt and observable behavior as the proper subject matter of psychology. Through the scientific study of behavior, it was hoped that laws of learning could be derived that would promote the prediction and control of behavior.
Ivan Pavlov (1870-1937) and Classical Conditioning[8] and Classical Conditioning with Animals
Ivan Pavlov was a Russian physiologist interested in studying digestion. As he recorded the amount of salivation his laboratory dogs produced as they ate, he noticed that they began to salivate before the food arrived as the researcher walked down the hall and toward the cage. One possible explanation for this phenomenon would be that the dog learned that food comes after the bell.
Pavlov began to experiment with this concept of classical conditioning. He began to ring a bell, for instance, prior to introducing the food. Sure enough, after making this connection several times, the dogs could be made to salivate to the sound of a bell. Once the bell had become an event to which the dogs had learned to salivate, it was called a conditioned stimulus. The act of salivating to a bell was a response that had also been learned, now termed in Pavlov’s jargon, a conditioned response. Notice that the response, salivation, is the same whether it is conditioned or unconditioned (unlearned or natural). What changed is the stimulus to which the dog salivates. One is natural (unconditioned) and one is learned (conditioned).
Summary of Classical Conditioning Process (Animals)
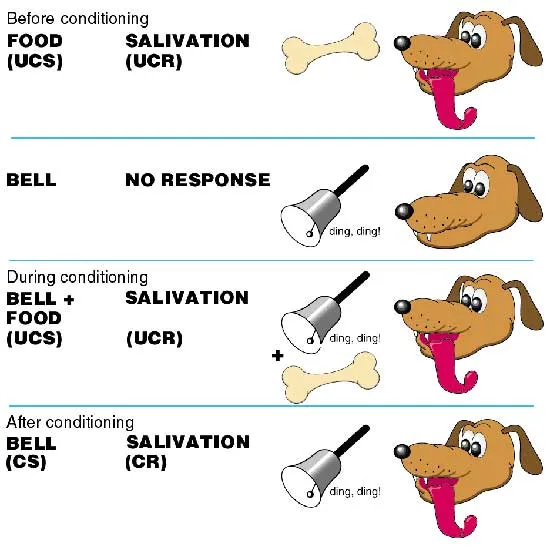
Pavlovian Conditioning of a dog to salivate upon hearing a bell.
To summarize, classical conditioning (later developed by Watson, 1913) involves learning to associate an unconditioned stimulus that already brings about a particular response (i.e., a reflex) with a new (conditioned) stimulus, so that the new stimulus brings about the same response.
The unconditioned stimulus (or UCS) is the object or event that originally produces the reflexive /natural response. The response to this is called the unconditioned response (or UCR). The neutral stimulus (NS) is a new stimulus that does not produce a response. Once the neutral stimulus has become associated with the unconditioned stimulus, it becomes a conditioned stimulus (CS). The conditioned response (CR) is the response to the conditioned stimulus.[9]
Now, let’s think about how classical conditioning is used on us. One of the most widespread applications of classical conditioning principles was brought to us by the psychologist, John B. Watson.[10]
John B. Watson (1878-1958) and Classical Conditioning[11] and Classical Conditioning in Humans

Watson believed that most of our fears and other emotional responses are classically conditioned. He had gained a good deal of popularity in the 1920s with his expert advice on parenting offered to the public. He tried to demonstrate the power of classical conditioning with his famous experiment with an 18-month-old boy named “Little Albert”. Watson sat Albert down and introduced a variety of seemingly scary objects to him: a burning piece of newspaper, a white rat, etc. But Albert remained curious and reached for all of these things. Watson knew that one of our only inborn fears is the fear of loud noises so he proceeded to make a loud noise each time he introduced one of Albert’s favorites, a white rat. After hearing the loud noise several times paired with the rat, Albert soon came to fear the rat and began to cry when it was introduced. Watson filmed this experiment for posterity and used it to demonstrate that he could help parents achieve any outcomes they desired, if they would only follow his advice. Watson wrote columns in newspapers and in magazines and gained a lot of popularity among parents eager to apply science to household order. [12]
Summary of Classical Conditioning Process (Humans)
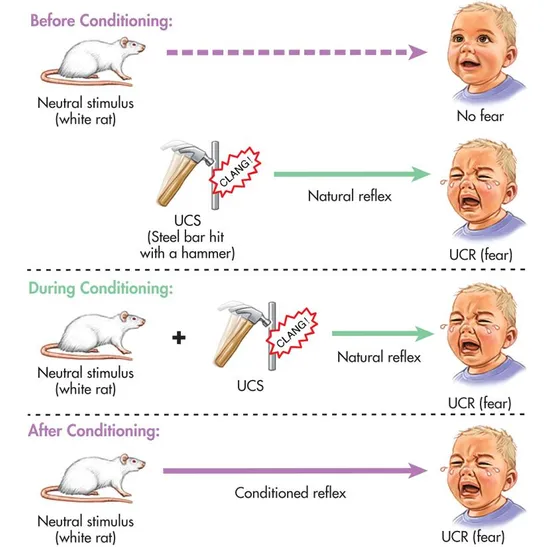
Watson’s conditioning of Little Albert to fear a white rat. [13]
Operant conditioning, on the other hand, looks at the way the consequences of a behavior increase or decrease the likelihood of a behavior occurring again. So, let’s look at this a bit more.[14]
B.F. Skinner (1904-1990) and Operant Conditioning[15] and Operant Conditioning in Animals and Humans

Skinner (1904-1990), who brought us the principles of operant conditioning, suggested that reinforcement is a more effective means of encouraging a behavior than is punishment. By focusing on strengthening desirable behavior, we have a greater impact than if we emphasize what is undesirable.
Reinforcement is the process by which a consequence increases the probability of a behavior that it follows. A reinforcer is a specific stimulus or situation that encourages the behavior that it follows. Intrinsic or primary reinforcers are reinforcers that have innate reinforcing qualities. These kinds of reinforcers are not learned and satisfy a biological need. Water, food, sleep, shelter, sex, pleasure, and touch, among others, are primary reinforcers. Swimming in a cool lake on a very hot day would be innately reinforcing because the water would cool the person off (a physical need), as well as provide pleasure. Extrinsic or secondary reinforcers have no inherent value and only have reinforcing qualities when linked with primary reinforcers. They can be traded in for what is ultimately desired. Praise, when linked to affection, is one example of a secondary reinforcer. Another example is money, which is only worth something when you can use it to buy other things—either things that satisfy basic needs (food, water, shelter—all primary reinforcers) or other secondary reinforcers. Extrinsic or secondary reinforcers are things that have a value not immediately understood.
Positive reinforcement occurs when the addition of a stimulus strengthens behavior. For example, positively reinforcing a child with the addition of a cookie for cleaning up will likely make encourage that behavior in the future. Negative reinforcement, on the other hand, occurs when removing a desired stimulus (or preventing access to it) strengthens behavior. For example, an alarm clock makes a very unpleasant, loud sound when it goes off in the morning. As a result, one gets up and turns it off. Therefore, getting up from bed is negatively reinforced through the termination of the aversive sound.
Punishmentis the process by which there decrease in the probability of behavior as a result of the consequence that follows it. Positive punishment occurs when the addition of an unpleasant or painful stimulus weakens behavior. For example, if a child is naughty and receives a spanking, the child will be less likely to misbehave in the future. Negative punishment, on the other hand, weakens a behavior through the removal of a desirable stimulus or preventing access to it. For example, a child who misbehaves and as a result has their favorite toy will be less likely to misbehave in the future. Punishment is often less effective than reinforcement for several reasons. It doesn’t indicate the desired behavior, it may result in suppressing rather than stopping a behavior, (in other words, the person may not do what is being punished when you’re around, but may do it often when you leave), and a focus on punishment can result in not noticing when the person does well.
Examples of Operant Conditioning Using Positive and Negative Reinforcement and Positive and Negative Punishers
| | POSITIVE
(Receive a Stimulus) |
NEGATIVE
(Stimulus Gets Taken Away) |
| REINFORCER
(Probability of Behavior Increases) |
Infant says “Mama” and mother claps her hands, smiles, and says, “very good, yes Mama!” The infant likes seeing the mother perform this way so continues to say “Mama.” | Infant’s diaper is wet or dirty, so infant cries. Someone comes and changes the diaper, thereby reducing the discomfort. The next time the child is uncomfortable, the child will cry. |
| PUNISHER
(Probability of Behavior Decreases) |
Child pulls the dog’s tail and the dog growls at the child. The child becomes frightened and does not pull the dog’s tail again. | Child behaves badly and his toy is taken away. The child learns that particular behavior is unacceptable and doesn’t want to lose the toy again, so the behavior is decreased or eliminated. |
Not all behaviors are learned through association or reinforcement. Many of the things we do are learned by watching others. This is addressed in social learning theory.[16]
Schedules of Reinforcement
Imagine a rat in a “Skinner box.” In operant conditioning, if no food pellet is delivered immediately after the lever is pressed then after several attempts the rat stops pressing the lever (how long would someone continue to go to work if their employer stopped paying them?). The behavior has been extinguished.
Behaviorists discovered that different patterns or schedules of reinforcement had different effects on the speed of learning and extinction. Ferster and Skinner (1957) devised different ways of delivering reinforcement and found that this had effects on
- The Response Rate – The rate at which the rat pressed the lever (i.e., how hard the rat worked).
- The Extinction Rate – The rate at which lever pressing dies out (i.e., how soon the rat gave up).
Skinner found that the type of reinforcement which produces the slowest rate of extinction (i.e., people will go on repeating the behavior for the longest time without reinforcement) is variable-ratio reinforcement. The type of reinforcement which has the quickest rate of extinction is continuous reinforcement.
| Response rate
Extinction rate |
slow | fast | |
| slow |
Variable Interval Reinforcement: Providing one correct response has been made, reinforcement is given after an unpredictable amount of time has passed, e.g., on average every 5 minutes. An example is a self-employed person being paid at unpredictable times. |
||
| medium |
Fixed Interval Reinforcement:One reinforcement is given after a fixed time interval providing at least one correct response has been made. An example is being paid by the hour. Another example would be every 15 minutes (half hour, hour, etc.) a pellet is delivered (providing at least one lever press has been made) then food delivery is shut off. |
Fixed Ratio Reinforcement:Behavior is reinforced only after the behavior occurs a specified number of times. e.g., one reinforcement is given after every so many correct responses, e.g., after every 5th response. For example, a child receives a star for every five words spelled correctly. |
|
| fast |
continuous reinforcementAn animal/human is positively reinforced every time a specific behavior occurs, e.g., every time a lever is pressed a pellet is delivered, and then food delivery is shut off. |
Variable Ratio Reinforcement:Behavior is reinforced after an unpredictable number of times. For examples gambling or fishing. |
Graphic Representation of Schedules of Reinforcement
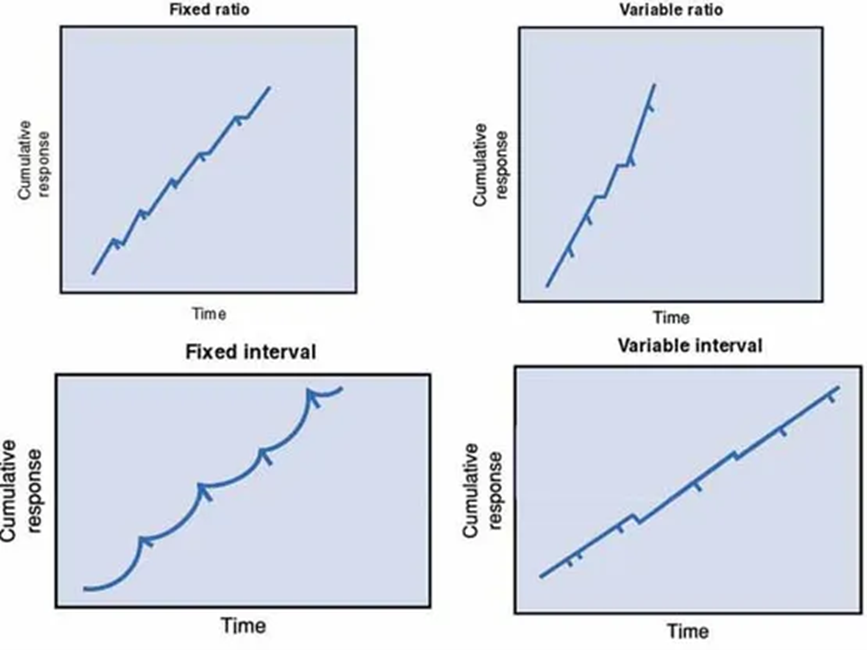
Each dash indicates the point where reinforcement is given. [18]
Albert Bandura (1925-2021) and Social Learning Theory[19] and Social Learning Theory

Albert Bandura is a leading contributor to social learning theory. He calls our attention to the ways in which many of our actions are not learned through conditioning; rather, they are learned by watching others (1977). Young children frequently learn behaviors through imitation.
Sometimes, particularly when we do not know what else to do, we learn by observing others model their behavior and then imitating or copying that behavior. A kindergartner on his or her first day of school might eagerly look at how others are acting and try to act the same way to fit in more quickly. Adolescents struggling with their identity rely heavily on their peers to act as role-models. Sometimes we do things because we’ve seen it pay off for someone else. They were operantly conditioned, but we engage in the behavior because we hope it will pay off for us as well. This is referred to as vicarious reinforcement (Bandura, Ross and Ross, 1963).
Bandura (1986) suggests that there is interplay between the environment and the individual. We are not just the product of our surroundings, rather we influence our surroundings. Parents not only influence their child’s environment, perhaps intentionally through the use of reinforcement, etc., but children influence parents as well. Parents may respond differently with their first child than with their fourth. Perhaps they try to be the perfect parents with their firstborn, but by the time their last child comes along they have very different expectations both of themselves and their child. Our environment creates us, and we create our environment. [20]
Cognitive Developmental Theories
Jean Piaget (1896-1980) and Theory of Cognitive Development[23]
Jean Piaget is one of the most influential cognitive theorists, and in the later modules we will discuss his work and his legacy in much more detail. Piaget was inspired to explore children’s ability to think and reason by watching his own children’s development. He was one of the first to recognize and map out the ways in which children’s thought differs from that of adults. His interest in this area began when he was asked to test the IQ of children and began to notice that there was a pattern in their wrong answers. He believed that children’s intellectual skills change over time through maturation. Children of differing ages interpret the world differently.
Piaget believed our desire to understand the world comes from a need for cognitive equilibrium. This is an agreement or balance between what we sense in the outside world and what we know in our minds. If we experience something that we cannot understand, we try to restore the balance by either changing our thoughts or by altering the experience to fit into what we do understand. Perhaps you meet someone who is very different from anyone you know. How do you make sense of this person? You might use them to establish a new category of people in your mind or you might think about how they are similar to someone else.
A schema or schemes are categories of knowledge. They are like mental boxes of concepts. A child has to learn many concepts. They may have a scheme for “under” and “soft” or “running” and “sour”. All of these are schema. Our efforts to understand the world around us lead us to develop new schema and to modify old ones.
One way to make sense of new experiences is to focus on how they are similar to what we already know. This is assimilation. So, the person we meet who is very different may be understood as being “sort of like my brother” or “his voice sounds a lot like yours.” Or a new food may be assimilated when we determine that it tastes like chicken!
Another way to make sense of the world is to change our mind. We can make a cognitive accommodation to this new experience by adding new schema. This food is unlike anything I’ve tasted before. I now have a new category of foods that are bitter-sweet in flavor, for instance. This is accommodation. Do you accommodate or assimilate more frequently? Children accommodate more frequently as they build new schema. Adults tend to look for similarity in their experience and assimilate. They may be less inclined to think “outside the box.”
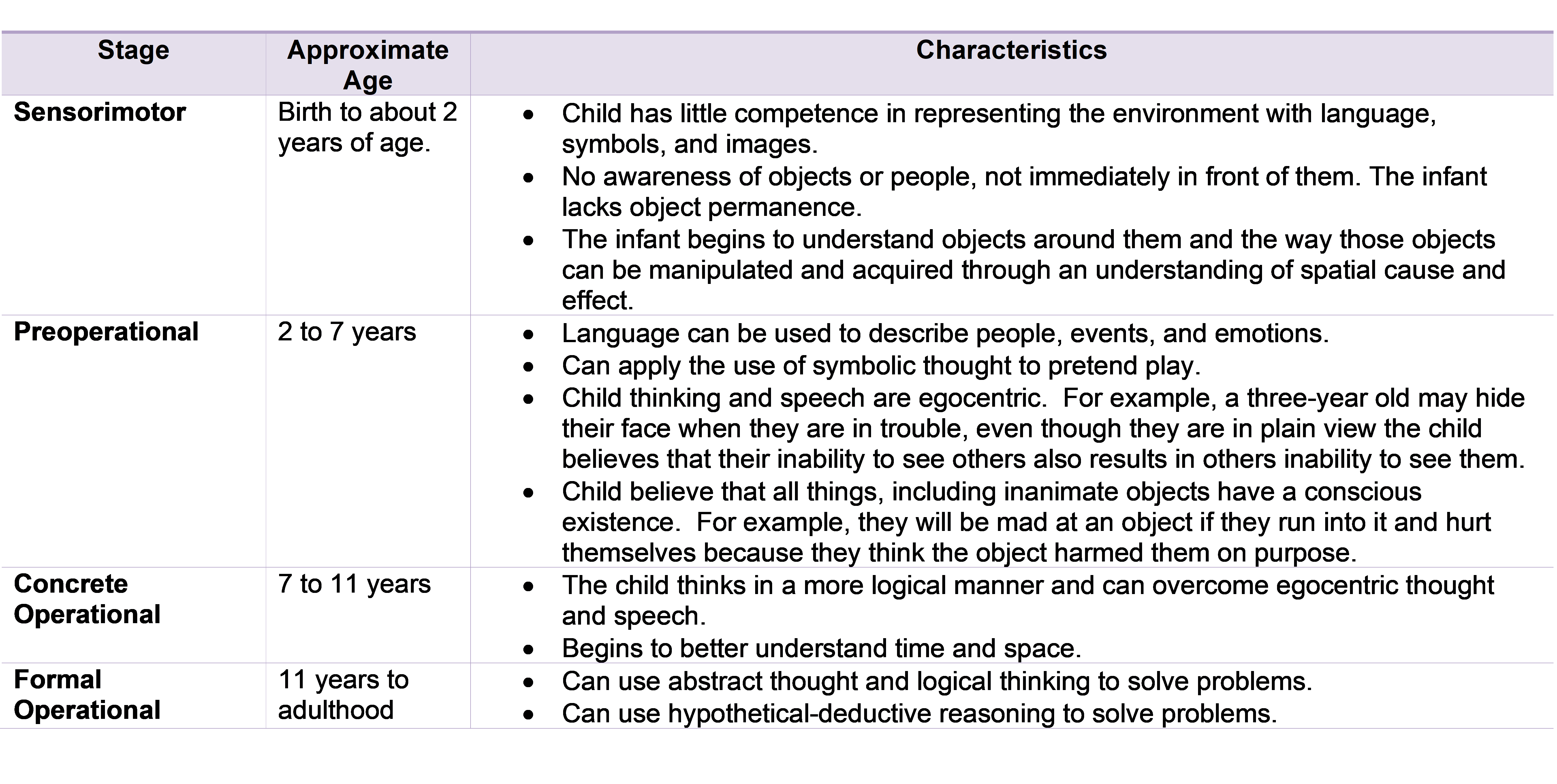
Piaget suggested different ways of understanding that are associated with maturation. He divided this understanding into the following four stages which will be discussed in much more detail in Chapter 7:
Piaget’s Stages of Cognitive Development [24]
Criticisms of Piaget’s Theory
Piaget has been criticized for overemphasizing the role that physical maturation plays in cognitive development and in underestimating the role that culture and interaction (or experience) plays in cognitive development. Looking across cultures reveals considerable variation in what children are able to do at various ages. Piaget may have underestimated what children are capable of given the right circumstances.[25]
Lev Vygotsky (1896-1934) and Sociocultural Theory[26]

Lev Vygotsky was a Russian psychologist who wrote in the early 1900s but whose work was discovered in the United States in the 1960s but became more widely known in the 1980s. Vygotsky differed with Piaget (this difference will be discussed in more detail in Chapter 7) in that he believed that a person not only has a set of abilities, but also a set of potential abilities that can be realized if given the proper guidance from others. His sociocultural theory emphasizes the importance of culture and interaction in the development of cognitive abilities. He believed that through guided participation known as scaffolding, with a teacher or capable peer, a child can learn cognitive skills within a certain range known as the zone of proximal development.[27]
Have you ever taught a child to perform a task? Maybe it was brushing their teeth or preparing food. Chances are you spoke to them and described what you were doing while you demonstrated the skill and let them work along with you all through the process. You gave them assistance when they seemed to need it, but once they knew what to do-you stood back and let them go. This is scaffolding and can be seen demonstrated throughout the world. This approach to teaching has also been adopted by educators. Rather than assessing students on what they are doing, they should be understood in terms of what they are capable of doing with the proper guidance. You can see how Vygotsky would be very popular with modern day educators.[28]
Comparing Piaget and Vygotsky
Vygotsky concentrated more on the child’s immediate social and cultural environment and his or her interactions with adults and peers. While Piaget saw the child as actively discovering the world through individual interactions with it, Vygotsky saw the child as more of an apprentice, learning through a social environment of others who had more experience and were sensitive to the child’s needs and abilities. We will elaborate on the two theories in later modules [29]
Information Processing
Information Processing is not the work of a single theorist but based on the ideas and research of several cognitive scientists studying how individuals perceive, analyze, manipulate, use, and remember information. This approach assumes that humans gradually improve in their processing skills; that is, cognitive development is continuous rather than stage-like. The more complex mental skills of adults are built from the primitive abilities of children. We are born with the ability to notice stimuli, store, and retrieve information. Brain maturation enables advancements in our information processing system. At the same time, interactions with the environment also aid in our development of more effective strategies for processing information.[30]
Urie Bronfenbrenner (1917-2005) and Ecological Systems Theory[31]
Bronfenbrenner offers us one of the most comprehensive theories of human development. Bronfenbrenner studied Freud, Erikson, Piaget, and learning theorists and believed that all those theories could be enhanced by adding the dimension of context. What is being taught and how society interprets situations depends on who is involved in the life of a child and on when and where a child lives. Bronfenbrenner’s ecological systems model explains the direct and indirect influences on an individual’s development.[32] The individual is impacted by several systems including:
- Microsystem includes the individual’s setting and those who have direct, significant contact with the person, such as parents or siblings. The input of those is modified by the cognitive and biological state of the individual as well. These influence the person’s actions, which in turn influence systems operating on him or her.
- Mesosystem includes the larger organizational structures, such as school, the family, or religion. These institutions impact the microsystems just described. The philosophy of the school system, daily routine, assessment methods, and other characteristics can affect the child’s self-image, growth, sense of accomplishment, and schedule thereby impacting the child, physically, cognitively, and emotionally.
- Exosystem includes the larger contexts of community. A community’s values, history, and economy can impact the organizational structures it houses. Mesosystems both influence and are influenced by the exosystem.
- Macrosystem includes the cultural elements, such as global economic conditions, war, technological trends, values, philosophies, and a society’s responses to the global community.
- Chronosystem is the historical context in which these experiences occur. This relates to the different generational time periods previously discussed, such as the baby boomers and millennials.
In sum, a child’s experiences are shaped by larger forces, such as the family, schools, religion, culture, and time period. Bronfenbrenner’s model helps us understand all the different environments that impact each one of us simultaneously. Despite its comprehensiveness, Bronfenbrenner’s ecological system’s theory is not easy to use. Taking into consideration all the different influences makes it difficult to research and determine the impact of all the different variables (Dixon, 2003). Consequently, psychologists have not fully adopted this approach, although they recognize the importance of the ecology of the individual.[33]
Bronfenbrenner’s Ecological Systems Theory[34]

Conclusion
Many early theories of human development were created and popularized in the early 1900s. These are referred to as stage theories because they present development as occurring in stages. The assumption is that once one stage is completed, a person moves into the next stage and that stages tend to occur only once. Some examples of stage theories that we will be studying include Freud’s psychosexual stages, Erikson’s psychosocial stages, and Piaget’s stages of cognitive development, to name a few.
These theories are appealing in a way because they provide the ability to predict what will happen next and they allow us to attribute behavior to a person’s being ‘in a stage’. These theories offered the security of understanding human behavior in a time of rapid change during industrialization in the early 1900s. Science seemed to be laying a predictable groundwork we could rely upon. But these early theories also implied that those who did not progress through stages in the predictable way were delayed somehow and this led to the idea that development had to occur in a patterned way.
Today we understand that development does not occur in a straight line. Sometimes we change in many directions depending on our experiences and surroundings. For example, there can be growth and decline in cognitive functioning at any age depending on nutrition, health, activity, and stimulation. And that both nature (heredity) and nurture (the environment) shape our abilities throughout life. Some things about us are continuous such as our temperament or sense of self, perhaps. And we may revisit a stage of life more than once. For instance, Erikson suggests that we struggle with trust as infants and then begin to focus more on independence or autonomy. But if we are in circumstances in which our independence is jeopardized, such as becoming physically dependent, we may struggle with trust again. Keep these thoughts in mind as we explore stage theories in our next lesson.
The study of human development is based on research. The next chapter looks at some of the different types of research methods used to understand development. In other words, how do we know what we know?[35]
Media Attributions
- Private: John Locke
- Private: Roussou
- Private: Image 4 Freud
- Private: Image 5 Iceburg Id Ego and Superego
- Private: Image 6 Freud’s Psychosexual Stages
- Private: Image7 Erikson
- Private: Image 8 Table Eriksons Psychosocial Theory
- Private: Item 9 Pavlov
- Private: Item 10 Classical Conditioning Chart
- Private: Item 11 Watson
- Private: Item 12 Classical Conditioning Human
- Private: Item 13 Skinner
- Private: Item 14 Schedules of Reinforcement
- Private: Item 15 Bandura
- Private: Item 16 Blurb on Bandura and Bobo Doll Experiment
- Private: Item 17 Piaget
- Private: Item 18B New Version of Piagetian Stages Chart
- Private: Item 19 Vygotsky
- Private: Item 20 Bronfenbrenner
- Private: Item 21 Brofenbrenner Ecological System
- Image of John Locke by Godfrey Kneller and is public domain ↵
- Image of Rousseau from Wikimedia Commons and is public domain ↵
- Image of Freud is public domain ↵
- Child Growth and Development: An Open Educational Resources Publication by College of the Canyons by Jennifer Paris, Antoinette Ricardo, and Dawn Richmond is licensed under CC BY 4.0 ↵
- McLeod, S. A. (2019, September 25). Id, ego and superego. Simply Psychology. https://www.simplypsychology.org/psyche.html. Licensed under CC BY NC ND 3.0 ↵
- Image from McLeod, S. A. (2019, September 25). Id, ego and superego. Simply Psychology. https://www.simplypsychology.org/psyche.html. Licensed under CC BY NC ND 3.0 Text by Maria Pagano ↵
- Image of Erikson is public domain ↵
- Image of Pavlov is in the public domain ↵
- Text and image by McLeod, S. A. (2018, October 08). Pavlov's dogs. Simply Psychology. https://www.simplypsychology.org/pavlov.html Licensed under CC BY NC ND 3.0 ↵
- Child Growth and Development: An Open Educational Resources Publication by College of the Canyons by Jennifer Paris, Antoinette Ricardo, and Dawn Richmond is licensed under CC BY 4.0 ↵
- Image of Watson is public domain ↵
- Child Growth and Development: An Open Educational Resources Publication by College of the Canyons by Jennifer Paris, Antoinette Ricardo, and Dawn Richmond is licensed under CC BY 4.0 ↵
- Image by McLeod, S. A. (2018, October 08). Pavlov's dogs. Simply Psychology. https://www.simplypsychology.org/pavlov.html Licensed under CC BY NC ND 3.0 ↵
- Child Growth and Development: An Open Educational Resources Publication by College of the Canyons by Jennifer Paris, Antoinette Ricardo, and Dawn Richmond is licensed under CC BY 4.0 ↵
- Image of Skinner is public domain ↵
- Child Growth and Development: An Open Educational Resources Publication by College of the Canyons by Jennifer Paris, Antoinette Ricardo, and Dawn Richmond is licensed under CC BY 4.0 (modified by Maria Pagano and Marie Parnes) ↵
- McLeod, S. A. (2018, January, 21). Skinner - operant conditioning. Simply Psychology. https://www.simplypsychology.org/operant-conditioning.html Licensed under CC BY NC ND 3.0 ↵
- McLeod, S. A. (2018, January, 21). Skinner - operant conditioning. Simply Psychology. https://www.simplypsychology.org/operant-conditioning.html Licensed under CC BY NC ND 3.0 ↵
- Image of Albert Bandura is licensed under CC BY-SA 4.0 ↵
- Exploring Behavior by Lumen Learning is licensed under CC BY 4.0Rasmussen, Eric (2017, Oct 19). Screen Time and Kids: Insights from a New Report. Retrieved from https://www.pbs.org/parents/thrive/screen-time-and-kids-insights-from-a-new-report ↵
- Child Growth and Development: An Open Educational Resources Publication by College of the Canyons by Jennifer Paris, Antoinette Ricardo, and Dawn Richmond is licensed under CC BY 4.0 ↵
- Child Growth and Development: An Open Educational Resources Publication by College of the Canyons by Jennifer Paris, Antoinette Ricardo, and Dawn Richmond is licensed under CC BY 4.0 ↵
- Image is in the public domain and taken from Child Growth and Development: An Open Educational Resources Publication by College of the Canyons by Jennifer Paris, Antoinette Ricardo, and Dawn Richmond is licensed under CC BY 4.0 ↵
- Original document created by Jordy von Hippel and taken from her Developmental Psychology WordPress Blog. No copyright information provided on site. Material updated by Maria Pagano ↵
- Lecture Transcript: Developmental Theories by Lumen Learning is licensed under CC BY 4.0 (modified by Jennifer Paris) ↵
- Image by The Vigotsky Project is licensed under CC BY-SA 3.0 ↵
- Exploring Cognition by Lumen Learning is licensed under CC BY 4.0 ↵
- Exploring Cognition by Lumen Learning is licensed under CC BY 4.0 ↵
- Children’s Development by Ana R. Leon is licensed under CC BY 4.0 ↵
- Lifespan Development: A Psychological Perspective 2nd Edition by Martha Lally and Suzanne Valentine-French is licensed under CC BY-NC-SA 3.0 ↵
- Image by Marco Vicente González is licensed under CC BY-SA 4.0 ↵
- Child Growth and Development: An Open Educational Resources Publication by College of the Canyons by Jennifer Paris, Antoinette Ricardo, and Dawn Richmond is licensed under CC BY 4.0 ↵
- Lifespan Development: A Psychological Perspective 2nd Edition by Martha Lally and Suzanne Valentine-French is licensed under CC BY-NC-SA 3.0 ↵
- Image by Ian Joslin is licensed under CC BY 4.0 ↵
- Lecture Transcript: Lifespan Development by Lumen Learning is licensed under CC BY 4.0 (modified by Maria Pagano) ↵
A child’s status among their peers will influence their membership in peer groups and their ability to make friends. Sociometric status is a measurement that reflects the degree to which someone is liked or disliked by their peers as a group. In developmental psychology, this system has been used to examine children's status in peer groups, its stability over time, the characteristics that determine it, and the long-term implications of one's popularity or rejection by peers.
The most commonly used sociometric system, developed by Coie & Dodge (1988), asks children to rate how much they like or dislike each of their classmates and uses these responses to classify them into five groups.

Figure 11.3.1. Sociometric peer statuses.
Popular adolescents are those liked by many of their peers and disliked by few. These individuals are skilled at social interactions and maintain positive peer relationships. They tend to be cooperative, friendly, sociable, and sensitive to others. They are capable of being assertive without being aggressive, thus can get what they want without harming others. Among this group, there may be distinct levels of popularity:
- Accepted teens are the most common sub-group among the popular. While they are generally well-liked, they are not as magnetic as the very popular kids.
- Very popular teens are highly charismatic and draw peers to them.
Rejected teens are designated as rejected if they receive many negative nominations and few positive nominations. These individuals often have poor academic performance and more behavior problems in school. They are also at higher risk for delinquent behaviors and legal problems. These kids are more likely to be diagnosed with ADHD, conduct disorder, and substance abuse. They tend to be isolated, lonely and are at risk for depression. Rejected youth can be categorized into two types:
- Aggressive-rejected teens display hostile and threatening behavior, are physically aggressive, and disruptive. They may bully others, withhold friendship, ignore and exclude others. While they are lacking, they tend to overestimate their social competence.
- Withdrawn-rejected teens are socially withdrawn, wary, timid, anxious in social situations, and lack confidence. They are at risk of being bullied.
Individuals that are liked by many peers, but also dislike by many are designated as controversial. This group may possess characteristics of both the popular and the rejected group. These individuals tend to be aggressive, disruptive, and prone to anger. However, they may also be cooperative and social. They are often socially active and a good group leader. Their peers often view them as arrogant and snobbish.
The neglected teens are designated as neglected if they receive few positive or negative nominations. These children are not especially liked or disliked by peers and tend to go unnoticed. As a result, they may be isolated and especially avoid confrontation or aggressive interactions. This group does tend to do well academically.
Finally, the average teens are designated as such because they receive an average number of both positive and negative nominations. They are liked by a small group of peers, but not disliked by very many.

Figure 11.3.2. Sociometric peer statuses and characteristics.
Popularity
What makes an adolescent popular? Several physical, cognitive, and behavioral factors impact popularity. First, adolescents that are perceived to be physically attractive tend to be more popular among their peers. Cognitive traits matter too. Individuals that demonstrate higher intelligence and do well academically tend to be more liked. Also, those that can take another’s perspective and demonstrate social problem-solving skills are favored. Teens that can manage their emotions and behave appropriately gain higher status. Finally, teens like peers that are confident without being conceited.
Interventions
What can be done to help those adolescents that are not well-liked? For neglected teens, social skills training and encouraging them to join activities can help them become noticed by their peers and make friends. For rejected teens, they may need support to help with anger management, to overcome anxiety, and cope with depression. This group can also benefit from social skills training to learn social competence and gain confidence.
Culture
As you might imagine, peer relationships are shaped by a wide range of contextual factors, and their development is not universal across all environments. One of the most significant influences is culture, which plays a key role in shaping how children and adolescents form and maintain relationships with their peers.
For example, in cultures that emphasize individualism—such as the United States—peer relationships tend to be more intimate and emotionally expressive. U.S. students often form close, dyadic friendships that are highly influential in shaping their social and emotional development. These friendships typically involve high levels of self-disclosure, loyalty, and mutual support.
In contrast, in cultures that emphasize collectivism—such as Indonesia—peer relationships are often broader and more group-oriented. Indonesian students may interact with a wider network of peers, placing greater value on group harmony, cooperation, and shared responsibility rather than deep individual closeness. While these relationships may seem less emotionally intense from a Western perspective, they reflect a strong sense of belonging within the peer group.
These differences highlight how cultural values shape not only the structure of peer relationships but also the expectations, behaviors, and emotional expressions within them. Recognizing these cultural variations helps us understand that peer development is deeply embedded within social and cultural contexts.
Family
In addition to culture, family also plays an important role in shaping children's peer relationships. Parents and caregivers can exert both direct and indirect influences. Directly, families influence who children associate with—for example, by arranging playdates or enrolling them in specific schools or activities. Indirectly, the neighborhood a family chooses can shape the peer group available to the child, especially in early and middle childhood, when friendships are often formed based on physical proximity.
Families also influence peer relationships through their impact on children’s social skills and behavior. Children observe how their parents interact with others and often model these behaviors. Furthermore, parenting styles that support socioemotional development—such as warm, responsive caregiving—are associated with children who possess better social skills, emotional regulation, and empathy (Moroni et al., 2019). These skills, in turn, enhance children's ability to build and maintain positive peer relationships.
Social Media
Finally, with the rise of technology and social media, peer relationships have undergone significant transformation. Social media increases the frequency and immediacy of peer interactions, making it easier for children and adolescents to stay connected. This can have positive effects, such as providing immediate social support, but may also lead to negative outcomes, like increased co-rumination or social comparison. Moreover, social media enables the formation of entirely online friendships, expanding the peer network beyond school and neighborhood boundaries. As a result, peer relationships are no longer limited by geographical proximity and are increasingly shaped by the digital environment, which can both enhance and complicate children's social experiences.
Impact of peer relationship
Throughout this book, we have emphasized the importance of peers in children’s development. Just like the family, peer relationships play a critical role across multiple domains of development. In fact, as children grow older—particularly after entering the formal school system—peer relationships become increasingly influential. Peers impact development in many areas, especially on their cognitive and socioemotional development.
As discussed in the section on academic achievement, peer influence plays a significant role in children’s learning. Participation in structured learning environments—such as collaborative study groups or classroom-based peer interactions—is positively associated with academic success. These settings not only reinforce academic skills but also foster motivation and engagement. As children mature, they become more likely to seek academic support from peers rather than family members, highlighting the growing importance of peer networks in educational contexts.
In addition to cognitive development, positive peer relationships are crucial for socioemotional development. Through peer interactions, children learn to navigate social dynamics, resolve conflicts, practice cooperation, and regulate their emotions. These experiences help them build essential social skills that contribute to emotional resilience and interpersonal competence. Children with supportive peer relationships tend to be more emotionally stable, exhibit higher self-esteem, and report greater life satisfaction.
Conversely, children who experience peer rejection or social exclusion are at greater risk for emotional difficulties. Repeated rejection or bullying can lead to heightened stress, which may contribute to serious consequences such as anxiety, depression, and poor academic outcomes. Therefore, fostering healthy peer relationships is essential for promoting well-rounded development and long-term well-being.
A child’s status among their peers will influence their membership in peer groups and their ability to make friends. Sociometric status is a measurement that reflects the degree to which someone is liked or disliked by their peers as a group. In developmental psychology, this system has been used to examine children's status in peer groups, its stability over time, the characteristics that determine it, and the long-term implications of one's popularity or rejection by peers.
The most commonly used sociometric system, developed by Coie & Dodge (1988), asks children to rate how much they like or dislike each of their classmates and uses these responses to classify them into five groups.
Figure 11.3.1. Sociometric peer statuses.
Popular students are those liked by many of their peers and disliked by few. These individuals are skilled at social interactions and maintain positive peer relationships. They tend to be cooperative, friendly, sociable, and sensitive to others. They are capable of being assertive without being aggressive, thus can get what they want without harming others. Among this group, there may be distinct levels of popularity:
- Accepted students are the most common sub-group among the popular. While they are generally well-liked, they are not as magnetic as the very popular kids.
- Very popular students are highly charismatic and draw peers to them.
Rejected students are designated as rejected if they receive many negative nominations and few positive nominations. These individuals often have poor academic performance and more behavior problems in school. They are also at higher risk for delinquent behaviors and legal problems. These kids are more likely to be diagnosed with ADHD, conduct disorder, and substance abuse. They tend to be isolated, lonely and are at risk for depression. Rejected youth can be categorized into two types:
- Aggressive-rejected students display hostile and threatening behavior, are physically aggressive, and disruptive. They may bully others, withhold friendship, ignore and exclude others. While they are lacking, they tend to overestimate their social competence.
- Withdrawn-rejected students are socially withdrawn, wary, timid, anxious in social situations, and lack confidence. They are at risk of being bullied.
Individuals that are liked by many peers, but also dislike by many are designated as controversial. This group may possess characteristics of both the popular and the rejected group. These individuals tend to be aggressive, disruptive, and prone to anger. However, they may also be cooperative and social. They are often socially active and a good group leader. Their peers often view them as arrogant and snobbish.
The neglected students are designated as neglected if they receive few positive or negative nominations. These children are not especially liked or disliked by peers and tend to go unnoticed. As a result, they may be isolated and especially avoid confrontation or aggressive interactions. This group does tend to do well academically.
Finally, the average students are designated as such because they receive an average number of both positive and negative nominations. They are liked by a small group of peers, but not disliked by very many.
Figure 11.3.2. Sociometric peer statuses and characteristics.
Popularity
What makes an adolescent popular? Several physical, cognitive, and behavioral factors impact popularity. First, adolescents that are perceived to be physically attractive tend to be more popular among their peers. Cognitive traits matter too. Individuals that demonstrate higher intelligence and do well academically tend to be more liked. Also, those that can take another’s perspective and demonstrate social problem-solving skills are favored. Teens that can manage their emotions and behave appropriately gain higher status. Finally, teens like peers that are confident without being conceited.
Interventions
What can be done to help those adolescents that are not well-liked? For neglected teens, social skills training and encouraging them to join activities can help them become noticed by their peers and make friends. For rejected teens, they may need support to help with anger management, to overcome anxiety, and cope with depression. This group can also benefit from social skills training to learn social competence and gain confidence.
Gender Development Theories
Gender refers to the socially constructed roles, behaviors, expressions, and identities associated with being male, female, or non-binary. It differs from sex, which is a biological term referring to physical and reproductive characteristics. Gender plays a significant role in our daily lives, shaping how we see ourselves and others. Multiple theories have been proposed to explain how children come to understand gender and how it becomes a central dimension for categorizing people and even objects.
Intergroup Theory
Intergroup theory suggests that while young children can perceive gender differences, they do not automatically attach meaning or stereotypes to those differences. However, adults often use gendered language and emphasize gender distinctions, which signals to children that gender is an important category. Over time, this emphasis leads children to form stereotypes based on gender. For example, a young girl may notice differences between herself and her brother, but she might not see those differences as meaningful unless her parents treat them differently—for instance, assigning her brother physical chores like mowing the lawn while she is asked to do indoor tasks like washing dishes.
Gender Schema Theory
Gender schema theory, rooted in Piaget’s cognitive developmental theory, views children as active learners who build mental frameworks—or schemas—to understand gender as a social category. Children observe and categorize behaviors, roles, and attributes associated with gender, and over time, they assimilate new information into these schemas or adjust them through accommodation. This process helps refine their understanding of what is considered "appropriate" for each gender based on social input.
Social Learning Theory
Social learning theory, drawing from behaviorist principles, proposes that children learn gender roles through modeling, reinforcement, and punishment. Children observe the behaviors of adults and peers and imitate those they see as aligned with their own gender. They then adjust their behavior based on the feedback they receive. For example, if a young boy paints his nails like his mother and is punished or teased for it, he may internalize the idea that nail polish is not appropriate for boys, thus shaping his understanding of gender roles.
Throughout this book, we have mentioned the importance of peers. Just like family, peer relationship plays an important role in our development. Actually, as children gets older, especially after they entered the formal school system, peer relationship becomes more and more impactful. Peer relationship influences children's development in many dimensions but we will focus on their influence on children's cognitive development and socioemotional development.
Cognitive Development
As we discussed in the academic achievement, peers play an important role in children's academic achievement. Being part of a structured learning community, such as a study group is positively associated with children's academic performance. As children grows older, they are more and morel ik
Influence of family on children
The influence of family on children’s development is both profound and long-lasting. For instance, the quality of attachment formed in infancy can predict socioemotional outcomes well into adulthood (Groh & Fearon, 2017). Children who have a secure and positive relationship with their caregivers are more likely to develop strong social-emotional skills, display prosocial behavior, form high-quality friendships, and be well-liked by peers. In contrast, children who lack a supportive caregiver relationship are at greater risk for difficulties in these areas.
Parental influence extends beyond socioemotional development and plays a crucial role in shaping children’s cognitive growth as well. The home environment and parents’ attitudes can significantly impact a child’s learning. For example, research has shown that children whose parents are anxious or avoidant about math tend to perform worse in the subject, compared to those whose parents express confidence and a positive attitude toward math (Casada et al., 2015) . This highlights the powerful role that parental beliefs and behaviors play in shaping children's academic outcomes.
While peers become increasingly important as children grow older, family continues to play a crucial role in children's development throughout middle childhood and adolescence. The influence of caregivers remains strong, shaping children's emotional well-being, values, academic motivation, and overall development. It is important to recognize the enduring impact of the family environment, and caregivers should strive to provide supportive, responsive, and nurturing conditions that promote healthy growth and adjustment during these formative years.
 As mentioned previously, Gender identity is one’s self-conception of their gender. Sex is the term to refer to the biological differences between males and females, such as the genitalia and genetic differences. While gender refers to the socially constructed characteristics of women and men, such as norms, roles, and relationships between groups of women and men. Cisgender is an umbrella term used to describe people whose sense of personal identity and gender corresponds with their birth sex, while transgender is a term used to describe people whose sense of personal identity does not correspond with their birth sex.
As mentioned previously, Gender identity is one’s self-conception of their gender. Sex is the term to refer to the biological differences between males and females, such as the genitalia and genetic differences. While gender refers to the socially constructed characteristics of women and men, such as norms, roles, and relationships between groups of women and men. Cisgender is an umbrella term used to describe people whose sense of personal identity and gender corresponds with their birth sex, while transgender is a term used to describe people whose sense of personal identity does not correspond with their birth sex.
Gender expression, or how one demonstrates gender (based on traditional gender role norms related to clothing, behavior, and interactions), can be feminine, masculine, androgynous, or somewhere along a spectrum. Many adolescents use their analytic, hypothetical thinking to question traditional gender roles and expression. If their genetically assigned sex does not line up with their gender identity, they may refer to themselves as transgender, non-binary, or gender-nonconforming.
Fluidity and uncertainty regarding sex and gender are especially common during early adolescence when hormones increase and fluctuate, creating a difficulty of self-acceptance and identity achievement (Reisner et al., 2016). Gender identity is becoming an increasingly prolonged task as attitudes and norms regarding gender keep changing. The roles appropriate for males and females are evolving, and some adolescents may foreclose on a gender identity as a way of dealing with this uncertainty by adopting more stereotypic male or female roles (Sinclair & Carlsson, 2013). Those that identify as transgender or ‘other’ face even more significant challenges.
Biological Approach to Gender Identity Development
The biological approach explores how gender identity development is influenced by genetics, biological sex characteristics, brain development, and hormone exposure.
Humans usually have 23 pairs of chromosomes, each containing thousands of genes that govern various aspects of our development. The 23rd pair of chromosomes are called the sex chromosomes. This pair determines a person’s sex, among other functions. Most often, if a person has an XX pair, they will develop into a female, and if they have an XY pair, then they will be male.
Around the sixth week of prenatal development, the SRY gene on the Y chromosome signals the body to develop as a male. This chemical signal triggers a cascade of other hormones that will tell the gonads to develop into testes. If the embryo does not have a Y or the if, for some reason, the SRY gene is missing or not activate, then the embryo will develop female characteristics. The baby is born and lives as a female, but genetically her chromosomes are XY. Rat studies have found that the reverse is also possible. Researchers implanted the SRY gene in rats with XX chromosomes, and the result was male baby mice.
Individuals with atypical chromosomes may also develop differently than their typical XX or XY counterparts. These chromosomal abnormalities include syndromes where a person may have only one sex chromosome or three sex chromosomes. Turner’s Syndrome is a condition where a female has only one X chromosome (XO). This missing chromosome results in a female external appearance but lacking ovaries. These XO females do not mature through puberty like XX females and they may also have webbed skin around the neck. Cognitively, these females tend to have high verbal skills, poor spatial and math skills, and poor social adjustment.
Klinefelter’s Syndrome is a condition where a male has an extra X chromosome (XXY). This XXY combination results in male genitals, although their genitals may be underdeveloped even into adulthood. Even after puberty, they tend to have less body and facial hair and may develop breasts. From infancy, these children often have a passive, cooperative, and shy personality that remains into adulthood. Cognitively, they are often late to talk and have poor language and reading skills.
As we learned in the physical development chapter, sex hormones cause biological changes to the body and brain. While the same sex hormones are present in males and females, the amount of each hormone and the effect of that hormone on the body is different. Males have much higher levels of testosterone than females. In the womb, testosterone causes the development of male sex organs. It also impacts the hypothalamus, causing an enlarged sexually dimorphic nucleus, and results in the ‘masculinization’ of the brain. Around the same time, testosterone may contribute to greater lateralization of the brain, resulting in the two halves working more independently of each other. Testosterone also affects what we often consider male behaviors, such as aggression, competitiveness, visual-spatial skills, and higher sex drive.
Cognitive Approaches to Gender Identity Development
Cognitive Learning Theory
Cognitive learning theory states that children develop gender at their own levels. At each stage, the child thinks about gender characteristically. As a child moves forward through stages, their understanding of gender becomes more complex.
The following cognitive model, formulated by Kohlberg, asserts that children recognize their gender identity around age three but do not see it as relatively fixed until the ages of five to seven. This identity marker provides children with a schema, a set of observed or spoken rules for how social or cultural interactions should happen. Information about gender is gathered from the environment; thus, children look for role models to emulate maleness or femaleness as they grow.
Stage 1: Gender Labeling (2-3.5 years). The child can label their gender correctly.
Stage 2: Gender Stability (3.5-4.5 years). The child’s gender remains the same across time.
Stage 3: Gender Constancy (6 years). The child’s gender is independent of external features (e.g., clothing, hairstyle).
Once children form a basic gender identity, they start to develop gender schemas. These gender schemas are organized set of gender-related beliefs that influence behaviors. The formation of these schemas explains the process by which gender stereotypes become so psychologically ingrained in our society.
Gender Schema Theory
Sandra Bem’s Gender Schema Theory, rooted in Piaget’s cognitive developmental theory, views children as active learners who build mental frameworks—or schemas—to understand gender as a social category. Children observe and categorize behaviors, roles, and attributes associated with gender, and over time, they assimilate new information into these schemas or adjust them through accommodation. This process helps refine their understanding of what is considered "appropriate" for each gender based on social input. According to this theory, gender schemas can be organized into four general categories. The sex-type schema is the belief that gender matches biological sex. Sex-reversed schema is when gender is the opposite of biological sex. Possessing both masculine and feminine traits is an androgynous schema. While possessing few masculine or feminine traits is an undifferentiated schema.
Social Approaches to gender identity development
Social Learning Theory
Social Learning Theory is based on outward motivational factors that argue that if children receive positive reinforcement, they are motivated to continue a particular behavior. If they receive punishment or other indicators of disapproval, they are more motivated to stop that behavior. In terms of gender development, children receive praise if they engage in culturally appropriate gender displays and punishment if they do not. When aggressiveness in boys is met with acceptance or a “boys will be boys” attitude, but a girl’s aggressiveness earns them little attention, the two children learn different meanings for aggressiveness as it relates to their gender development. Thus, boys may continue being aggressive while girls may drop it out of their repertoire.
Intergroup Theory
Intergroup theory suggests that while young children can perceive gender differences, they do not automatically attach meaning or stereotypes to those differences. However, adults often use gendered language and emphasize gender distinctions, which signals to children that gender is an important category. Over time, this emphasis leads children to form stereotypes based on gender. For example, a young girl may notice differences between herself and her brother, but she might not see those differences as meaningful unless her parents treat them differently—for instance, assigning her brother physical chores like mowing the lawn while she is asked to do indoor tasks like washing dishes.
Transgender Identity Development
Individuals who identify with the role that is different from their biological sex are called transgender. Approximately 1.4 million U.S. adults or .6% of the population are transgender, according to a 2016 report (Flores et al., 2016).
Transgender individuals may choose to alter their bodies through medical interventions such as surgery and hormonal therapy so that their physical being is better aligned with gender identity. They may also be known as male-to-female (MTF) or female-to-male (FTM). Not all transgender individuals choose to alter their bodies; many will maintain their original anatomy but may present themselves to society as another gender. This expression is typically done by adopting the dress, hairstyle, mannerisms, or other characteristics typically assigned to another gender. It is important to note that people who cross-dress or wear clothing that is traditionally assigned to a different gender is not the same as identifying as transgender. Cross-dressing is typically a form of self-expression, entertainment, or personal style, and it is not necessarily an expression against one’s assigned gender (APA 2008).
After years of controversy over the treatment of sex and gender in the American Psychiatric Association Diagnostic and Statistical Manual for Mental Disorders (Drescher 2010), the most recent edition, DSM-5, responded to allegations that the term “gender identity disorder” is stigmatizing by replacing it with “gender dysphoria.” Gender identity disorder as a diagnostic category stigmatized the patient by implying there was something “disordered” about them. Removing the word “disorder” also removed some of the stigmas while still maintaining a diagnosis category that will protect patient access to care, including hormone therapy and gender reassignment surgery.
In the DSM-5, gender dysphoria is a condition of people whose gender at birth is contrary to the one with which they identify. For a person to be diagnosed with gender dysphoria, there must be a marked difference between the individual’s expressed/experienced gender and the gender others would assign him or her, and it must continue for at least six months. In children, the desire to be of the other gender must be present and verbalized (APA, 2013). Changing the clinical description may contribute to greater acceptance of transgender people in society. A 2017 poll showed that 54% of Americans believe gender is determined by sex at birth, and 32% say society has “gone too far” in accepting transgender people; views are sharply divided along political and religious lines (Salam, 2018).
Many psychologists and the transgender community are now advocating an affirmative approach to transgender identity development. This approach advocates that gender non-conformity is not a pathology but a normal human variation. Gender non-conforming children do not systemically need mental health treatment if they are not “pathological.” However, care-givers of gender non-conforming children can benefit from a mixture of psycho-educational and community-oriented interventions. Some children or teens may benefit from counseling or other interventions to help them cope with familial or societal reactions to their gender-nonconformity.
Studies show that people who identify as transgender are twice as likely to experience assault or discrimination as non-transgender individuals; they are also one and a half times more likely to experience intimidation (National Coalition of Anti-Violence Programs 2010; Giovanniello, 2013). Trans women of color are most likely to be victims of abuse. There are also systematic aggressions, such as “deadnaming,” (whereby trans people are referred to by their birth name and gender), laws restricting transpersons from accessing gender-specific facilities (e.g., bathrooms), or denying protected-class designations to prevent discrimination in housing, schools, and workplaces. Organizations such as the National Coalition of Anti-Violence Programs and Global Action for Trans Equality work to prevent, respond to and end all types of violence against transgender and homosexual individuals. These organizations hope that by educating the public about gender identity and empowering transgender individuals, this violence will end.
Like other domains of identity, stage models for transgender identity development have helped describe a typical progression in identity formation. Lev’s Transgender Emergence Model looks at how trans people come to understand their identity. Lev is working from a counseling/therapeutic point of view, thus this model talks about what the individual is going through and the responsibility of the counselor.
Stage 1: Awareness. In this first stage of awareness, gender-variant people are often in great distress; the therapeutic task is the normalization of the experiences involved in emerging as transgender.
Stage 2: Seeking Information/Reaching Out. In the second stage, gender-variant people seek to gain education and support about transgenderism; the therapeutic task is to facilitate linkages and encourage outreach.
Stage 3: Disclosure to Significant Others. The third stage involves the disclosure of transgenderism to significant others (spouses, partners, family members, and friends); the therapeutic task involves supporting the transgender person’s integration in the family system.
Stage 4: Exploration (Identity & Self-Labeling). The fourth stage involves the exploration of various (transgender) identities; the therapeutic task is to support the articulation and comfort with one’s gendered identity.
Stage 5: Exploration (Transition Issues & Possible Body Modification). The fifth stage involves exploring options for transition regarding identity, presentation, and body modification; the therapeutic task is the resolution of the decision and advocacy toward their manifestation.
Stage 6: Integration (Acceptance & Post-Transition Issues). In the sixth stage, the gender-variant person can integrate and synthesize (transgender) identity; the therapeutic task is to support adaptation to transition-related issues.
As we previously discussed, gender is distinct from sex. Gender refers to the social, psychological, cultural, and behavioral traits associated with being male, female, or another gender identity. Sex, in contrast, refers to biological characteristics, such as chromosomes, hormones, and reproductive anatomy. As children’s gender identity continues to develop, their understanding of the traits, roles, and expectations associated with different genders also evolves over time.
In general, younger children tend to hold rigid gender stereotypes, but this rigidity often decreases as they enter middle childhood. For example, one study found that while only 33.8% of 5-year-olds believed that objects like vacuum cleaners were for both men and women, that number increased to 87.8% among 11-year-olds (Banse et al., 2010). However, this flexibility may decline again during adolescence, a time when youth begin exploring identity more deeply and often conform more closely to traditional gender roles. A study by Alferi and colleagues (1996) found that gender flexibility peaked in grades 7–8 and declined afterward, suggesting a return to more rigid views during later adolescence.
Measuring gender stereotypes
Gender stereotypes are commonly measured by assessing whether youth categorize certain attributes as male- or female-typical (i.e., gender stereotypes) and whether they view it as acceptable for both genders to express those traits (i.e., gender flexibility). In recent years, researchers have also turned to implicit measures such as the Implicit Association Test (IAT) to capture unconscious gender biases. In these tasks, participants categorize words or images related to gender (e.g., "man," "woman") and domains (e.g., "math," "language"). In congruent trials, gender-stereotypical pairings are grouped together (e.g., male/math), while in incongruent trials, non-stereotypical pairings are grouped (e.g., female/math). If participants have implicit stereotypes (e.g., associating men more strongly with math), they tend to respond more slowly in the incongruent trials. Research has consistently shown that such implicit biases are common in both adolescents and adults.
Video 11.
What influences gender stereotype?
Multiple factors contribute to the development of gender stereotypes, including family, media, and peers. Families, particularly fathers, often reinforce traditional gender roles, sometimes unconsciously. For example, boys are typically encouraged to be more independent and are often granted more autonomy than girls at an early age. These expectations extend to academic domains as well. One study found that when parents believed girls should be better at language arts and boys at math, their daughters internalized these beliefs—resulting in lower math performance and reduced enrollment in advanced STEM courses (Aidy et al., 2021).
Social media and peer influence also play a powerful role in shaping gender perceptions during adolescence. Social media often promotes narrow ideals, such as unrealistic body standards for girls, which can increase body dissatisfaction and reinforce gendered expectations. Similarly, peer influence can strengthen traditional gender role beliefs. A study of Belgian adolescents found that those with more same-sex friendships and higher levels of peer pressure were more likely to adopt traditional gender attitudes during early adolescence (Halimi et al., 2020).
Middle childhood and adolescence are critical periods for identity exploration, including gender identity and beliefs. During this time, children and adolescents form more complex understandings of themselves and others. Therefore, it is crucial for families and schools to foster supportive environments that encourage gender flexibilityand challenge harmful stereotypes. Doing so can promote healthier development and reduce stress related to rigid or limiting gender expectations.
Learning Objectives
- Describe changes in peer relationships during middle childhood and adolescence
- Identify the sociometric peer statuses and characteristics of each
- Explain the types of bullying and factors that contribute to bullying behavior
- Describe the developmental benefits of dating
- Explain teen dating violence and factors that contribute to this behavior
Parent-child relationships are not the only significant relationships in a child’s life. Peer relationships are also important. Social interaction with another child who is similar in age, skills, and knowledge provokes the development of many social skills that are valuable for the rest of life (Bukowski, Buhrmester, & Underwood, 2011). In peer relationships, children learn how to initiate and maintain social interactions with other children. They learn skills for managing conflicts, such as turn-taking, compromise, and bargaining. Through these experiences, children develop friendships that provide additional sources of security and support to those provided by their parents. These relationships become even more prominent during adolescence.
Learning Objectives
- Describe changes in peer relationships during middle childhood and adolescence
- Explain the impact of peer relationship on youth's development
- Identify the sociometric peer statuses and characteristics of each
- Explain the types of bullying and factors that contribute to bullying behavior
- Describe the developmental benefits of dating
- Explain teen dating violence and factors that contribute to this behavior
Parent-child relationships are not the only significant relationships in a child’s life. Peer relationships are also important. Social interaction with another child who is similar in age, skills, and knowledge provokes the development of many social skills that are valuable for the rest of life (Bukowski, Buhrmester, & Underwood, 2011). In peer relationships, children learn how to initiate and maintain social interactions with other children. They learn skills for managing conflicts, such as turn-taking, compromise, and bargaining. Through these experiences, children develop friendships that provide additional sources of security and support to those provided by their parents. These relationships become even more prominent during adolescence.
Learning Objectives
- Differentiate between gender and sex
- Explain gender identity development through middle childhood and adolescence
- Compare and contrast the biological, cognitive, and social perspective on gender identity development
- Explain sexual identity development through middle childhood and adolescence
- Explain the development of gender stereotype and factors contributing to gender stereotype through middle childhood and adolescence
Gender refers to the social, psychological, cultural, and behavioral traits associated with being male, female, or another gender identity. As children's identity develops, their understanding of their own gender identity also changes. It is important to note that gender is a socially constructed term. As such, we do not born with understanding of gender identity or perceptions of what is "typical" and "atypical" of a specific gender. As children entered school system and as their sexuality develops, their understanding of gender as a category and their own gender identity also goes through changes. Family, social media, and peers all played
Learning Objectives
- Differentiate between gender and sex
- Explain gender identity development through middle childhood and adolescence
- Compare and contrast the biological, cognitive, and social perspective on gender identity development
- Explain sexual identity development through middle childhood and adolescence
- Explain the development of gender stereotype and factors contributing to gender stereotype through middle childhood and adolescence
Gender refers to the social, psychological, cultural, and behavioral traits associated with being male, female, or another gender identity. As children's identity develops, their understanding of their own gender identity also changes. It is important to note that gender is a socially constructed term. As such, we do not born with understanding of gender identity or perceptions of what is "typical" and "atypical" of a specific gender. As children entered school system and as their sexuality develops, their understanding of gender as a category and their own gender identity also goes through changes. Family, social media, and peers all played an important role in this development as well as their attitude towards their own gender and other genders. We will explore the different theories on the development of gender and sexual identity, how we form gender stereotype and what influences the development of our gender stereotype in this chapter.
This textbook incorporates content from the following openly licensed sources:
-
Arduini-Van Hoose, N. (2020). Adolescent psychology. Retrieved from https://adolescentpsychology.pressbooks.sunycreate.cloud. CC BY-NC-SA 4.0 license. Content has been modified and adapted to fit the structure of this book.
- Pagano, M. & Parnes, M. (2022). Infany and Child Development: From Conception through late childhood. Retrieved from https://pressbooks.cuny.edu/infantandchilddevelopmentcitytech/ CC BY-NC-SA 4.0 license. Content has been modified and adapted to fit the structure of this book.
This textbook incorporates content from the following openly licensed sources:
-
Arduini-Van Hoose, N. (2020). Adolescent psychology. Retrieved from https://adolescentpsychology.pressbooks.sunycreate.cloud. CC BY-NC-SA 4.0 license. Content has been modified and adapted to fit the structure of this book.
- Pagano, M. & Parnes, M. (2022). Infany and Child Development: From Conception through late childhood. Retrieved from https://pressbooks.cuny.edu/infantandchilddevelopmentcitytech/ CC BY-NC-SA 4.0 license. Content has been modified and adapted to fit the structure of this book.
Liu,Q. (2025). Adolescent psychology. Retrieved from https://adolescentpsychology.pressbooks.sunycreate.cloud. CC BY-NC-SA 4.0 license.
What is Open Science?
Open Science refers to a movement that aims to make scientific research, data, and publications freely accessible to everyone, promoting transparency, collaboration, and reproducibility to increase the accessibility and impact of scientific knowledge.
Why do we need Open Science?
First, making research studies and related information freely accessible is nice. For example, having this open-source textbook for your class probably saved you a lot of money. With the same mindset, making research findings freely accessible to everyone will allow everyone to benefit from the research study.
Another reason for the need of Open Science has something to do with the poor research practices that have been conducted in the past. A previous study aimed to replicate all the research findings conducted in some of the most prominent journals in Psychology. As listed in the table below, only 36% of the findings published in those top-tier journals were replicated. This is concerning because it could mean that the research findings that we trusted and believed in actually do not exist in real life.
| Journal | % Findings Replicated |
| Journal of Personality and Social Psychology: Social | 23 |
| Journal of Experimental Psychology: Learning, Memory, and Cognition | 48 |
| Psychological Science, social articles | 29 |
| Psychological Science, cognitive articles | 53 |
| Overall | 36 |
Table 3.8.1. Percentage of research findings from journals replicated
Some of the reason behind this lack of replicability are due to questionable research practices including:
Low Statistical Power:
Low statistical power occurs when a study includes too small a sample size to detect meaningful effects. For example, imagine a study that tracks the intelligence of 10 individuals from age 20 to 50 and concludes that people become more intelligent as they age. With only 10 participants, the sample is too small to draw reliable conclusions, and there’s a high chance that the result is due to random variation or a special case rather than a true trend. As a result, the findings cannot be generalized to the broader population.
P-Hacking:
P-hacking refers to manipulating data analysis in order to obtain statistically significant results, even when there is no real effect. This can involve practices like running multiple statistical tests and only reporting the ones that yield significant results. Why is this problematic? Imagine each test has a 5% chance of producing a false positive result. If you run two tests, there’s about a 10% chance of finding at least one false positive. If you run 20 tests, the likelihood of finding at least one significant result by chance alone becomes very high—even if no real effect exists. Unfortunately, it is not uncommon for researchers to conduct many tests but only report the significant ones, which misleads readers and distorts scientific understanding.
HARKing (Hypothesizing After Results are Known):
HARKing occurs when researchers formulate or change their hypothesis after seeing the results, and then present it as if it were their original prediction. For instance, suppose you initially hypothesize that eating ice cream before a test will improve performance. After collecting data, you find the opposite result—that performance worsens. Instead of reporting the original hypothesis, you revise it to say that you predicted the decline in performance. This practice is misleading, as it presents post-hoc reasoning as if it were an a priori prediction, giving a false impression of scientific foresight and increasing the risk of false conclusions.
Falsification of Results:
This refers to the deliberate fabrication or alteration of data to produce a desired outcome. It is one of the most serious violations of scientific integrity and can have wide-reaching consequences for public trust and future research.
Publication Bias:
Publication bias occurs when studies with significant results are more likely to be published than those with null or non-significant findings. This skews the body of published research and contributes to questionable practices like p-hacking, HARKing, and even falsification. For example, imagine 11 studies are conducted to examine whether eating ice cream before a test improves performance. Ten of these studies find no significant effect, while one does. Due to publication bias, only the one "positive" study gets published. As a result, readers—including the public and other researchers—may mistakenly believe there is strong evidence supporting the effect, when in fact the overall evidence suggests otherwise.
Toolboxes for Open Science
As defined above, Open Science refers to the movement aimed at making research studies and their findings openly accessible to everyone. There are several ways researchers can contribute to this effort and increase the transparency and accessibility of their work.
One approach is to share research materials, analysis code, and datasets publicly. This not only fosters collaboration but also makes it easier for other researchers to replicate and verify findings. Writing detailed methods sections is another important practice, as it ensures that others can accurately understand and reproduce the procedures used in the study.
Researchers can also engage in preregistration or submit a preregistered report. In both cases, the research plan—including hypotheses, study design, and analysis strategies—is documented and submitted before data collection begins. This helps prevent questionable practices like p-hacking and HARKing by holding researchers accountable to their original research questions and plans.
Finally, practices such as publishing preprints (early versions of papers shared before peer review) and choosing open access publishing options allow research findings to be shared freely with the broader community, without financial or technical barriers. These practices make research more inclusive and ensure that scientific knowledge is accessible to students, educators, practitioners, and the general public.
The previous sections describe research tools to assess development across the lifespan, as well as the ways that research designs can be used to track age-related changes and development over time. Before you begin conducting developmental research, however, you must also be aware that testing individuals of certain ages (such as infants and children) or making comparisons across ages (such as children compared to teens) comes with its own unique set of challenges. In the final section of this module, let's look at some of the main issues that are encountered when conducting developmental research, namely ethical concerns, recruitment issues, and participant attrition.
Recruitment
An additional challenge in developmental science is participant recruitment. Recruiting university students to participate in adult studies is typically easy. Many colleges and universities offer extra credit for participation in research and have locations such as bulletin boards and school newspapers where research can be advertised. Unfortunately, young children cannot be recruited by making announcements in Introduction to Psychology courses, by posting ads on campuses, or through online platforms such as Amazon Mechanical Turk. Given these limitations, how do researchers go about finding infants and young children to be in their studies?
The answer to this question varies along multiple dimensions. Researchers must consider the number of participants they need and the financial resources available to them, among other things. Location may also be an important consideration. Researchers who need large numbers of infants and children may attempt to recruit them by obtaining infant birth records from the state, county, or province in which they reside. Some areas make this information publicly available for free, whereas birth records must be purchased in other areas (and in some locations birth records may be entirely unavailable as a recruitment tool). If birth records are available, researchers can use the obtained information to call families by phone or mail them letters describing possible research opportunities. All is not lost if this recruitment strategy is unavailable, however. Researchers can choose to pay a recruitment agency to contact and recruit families for them. Although these methods tend to be quick and effective, they can also be quite expensive. More economical recruitment options include posting advertisements and fliers in locations frequented by families, such as mommy-and-me classes, local malls, and preschools or daycare centers. Researchers can also utilize online social media outlets like Facebook, which allows users to post recruitment advertisements for a small fee. Of course, each of these different recruitment techniques requires IRB approval. And if children are recruited and/or tested in school settings, permission would need to be obtained ahead of time from teachers, schools, and school districts (as well as informed consent from parents or guardians).
And what about the recruitment of adults? While it is easy to recruit young college students to participate in research, some would argue that it is too easy and that college students are samples of convenience. They are not randomly selected from the wider population, and they may not represent all young adults in our society (this was particularly true in the past with certain cohorts, as college students tended to be mainly white males of high socioeconomic status). In fact, in the early research on aging, this type of convenience sample was compared with another type of convenience sample—young college students tended to be compared with residents of nursing homes! Fortunately, it didn't take long for researchers to realize that older adults in nursing homes are not representative of the older population; they tend to be the oldest and sickest (physically and/or psychologically). Those initial studies probably painted an overly negative view of aging, as young adults in college were being compared to older adults who were not healthy, had not been in school nor taken tests in many decades, and probably did not graduate high school, let alone college. As we can see, recruitment and random sampling can be significant issues in research with adults, as well as infants and children. For instance, how and where would you recruit middle-aged adults to participate in your research?
Attrition

Another important consideration when conducting research with infants and young children is attrition. Although attrition is quite common in longitudinal research in particular (see the previous section on longitudinal designs for an example of high attrition rates and selective attrition in lifespan developmental research), it is also problematic in developmental science more generally, as studies with infants and young children tend to have higher attrition rates than studies with adults. For example, high attrition rates in ERP (event-related potential, which is a technique to understand brain function) studies oftentimes result from the demands of the task: infants are required to sit still and have a tight, wet cap placed on their heads before watching still photographs on a computer screen in a dark, quiet room. In other cases, attrition may be due to motivation (or a lack thereof). Whereas adults may be motivated to participate in research in order to receive money or extra course credit, infants and young children are not as easily enticed. In addition, infants and young children are more likely to tire easily, become fussy, and lose interest in the study procedures than are adults. For these reasons, research studies should be designed to be as short as possible – it is likely better to break up a large study into multiple short sessions rather than cram all of the tasks into one long visit to the lab. Researchers should also allow time for breaks in their study protocols so that infants can rest or have snacks as needed. Happy, comfortable participants provide the best data.
Conclusions
Developmental Psychology is a fascinating field of study – but care must be taken to ensure that researchers use appropriate methods to examine human behavior, use the correct experimental design to answer their questions, and be aware of the special challenges that are part-and-parcel of developmental research. After reading this module, you should have a solid understanding of these various issues and be ready to think more critically about research questions that interest you. For example, what types of questions do you have about lifespan development? What types of research would you like to conduct? Many interesting questions remain to be examined by future generations of developmental scientists – maybe you will make one of the next big discoveries!
Did you know that as sales of ice cream increase, so does the overall rate of crime? Is it possible that indulging in your favorite flavor of ice cream could send you on a crime spree? Or, after committing a crime, do you think you might decide to treat yourself to a cone? There is no question that a relationship exists between ice cream and crime (e.g., Harper, 2013), but does one thing actually caused the other to occur.
It is much more likely that both ice cream sales and crime rates are related to the temperature outside. When the temperature is warm, there are lots of people out of their houses, interacting with each other, getting annoyed with one another, and sometimes committing crimes. Also, when it is warm outside, we are more likely to seek a refreshing treat like ice cream. How do we determine if there is indeed a relationship between two things? And when there is a relationship, how can we discern whether it is attributable to coincidence or causation? We do this through statistical analysis of the data. Which analysis we use will depend on several conditions outlined next.
Introduction to Statistical Thinking

Does drinking coffee actually increase your life expectancy? A recent study (Freedman, Park, Abnet, Hollenbeck, & Sinha, 2012) found that men who drank at least six cups of coffee a day had a 10% lower chance of dying (women 15% lower) than those who drank none. Does this mean you should pick up or increase your own coffee habit? Modern society has become awash in studies such as this; you can read about several such studies in the news every day. Conducting such a study well, and interpreting the results of such studies requires understanding basic ideas of statistics, the science of gaining insight from data. Key components to a statistical investigation are:
- Planning the study: Start by asking a testable research question and deciding how to collect data. For example, how long was the study period of the coffee study? How many people were recruited for the study, how were they recruited, and from where? How old were they? What other variables were recorded about the individuals? Were changes made to the participants’ coffee habits during the course of the study?
- Examining the data: What are appropriate ways to examine the data? What graphs are relevant, and what do they reveal? What descriptive statistics can be calculated to summarize relevant aspects of the data, and what do they reveal? What patterns do you see in the data? Are there any individual observations that deviate from the overall pattern, and what do they reveal? For example, in the coffee study, did the proportions differ when we compared the smokers to the non-smokers?
- Inferring from the data: What are valid statistical methods for drawing inferences “beyond” the data you collected? In the coffee study, is the 10%–15% reduction in risk of death something that could have happened just by chance?
- Drawing conclusions: Based on what you learned from your data, what conclusions can you draw? Who do you think these conclusions apply to? (Were the people in the coffee study older? Healthy? Living in cities?) Can you draw a cause-and-effect conclusion about your treatments? (Are scientists now saying that the coffee drinking is the cause of the decreased risk of death?)
Notice that the numerical analysis (“crunching numbers” on the computer) comprises only a small part of overall statistical investigation. In this section, you will see how we can answer some of these questions and what questions you should be asking about any statistical investigation you read about.
Video 2.6.1. Types of Statistical Studies explains the differences between correlational and experimental research.
https://assessments.lumenlearning.com/assessments/2708
Distributional Thinking
When data are collected to address a particular question, an important first step is to think of meaningful ways to organize and examine the data. Let's take a look at an example.
Example 1: Researchers investigated whether cancer pamphlets are written at an appropriate level to be read and understood by cancer patients (Short, Moriarty, & Cooley, 1995). Tests of reading ability were given to 63 patients. In addition, readability level was determined for a sample of 30 pamphlets, based on characteristics such as the lengths of words and sentences in the pamphlet. The results, reported in terms of grade levels, are displayed in Figure 2.6.2.

- Data vary. More specifically, values of a variable (such as reading level of a cancer patient or readability level of a cancer pamphlet) vary.
- Analyzing the pattern of variation, called the distribution of the variable, often reveals insights.
Addressing the research question of whether the cancer pamphlets are written at appropriate levels for the cancer patients requires comparing the two distributions. A naïve comparison might focus only on the centers of the distributions. Both medians turn out to be ninth grade, but considering only medians ignores the variability and the overall distributions of these data. A more illuminating approach is to compare the entire distributions, for example with a graph, as in Figure 2.6.3.
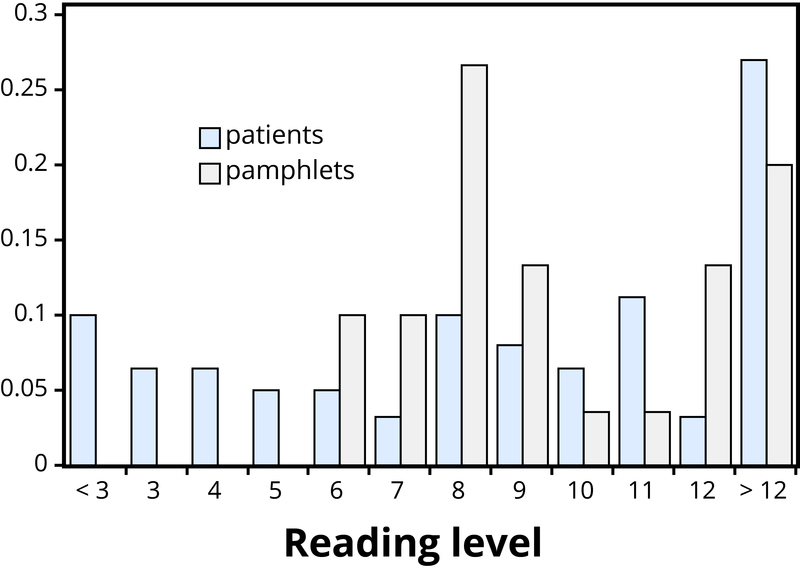
Figure 2.6.3 makes clear that the two distributions are not well aligned at all. The most glaring discrepancy is that many patients (17/63, or 27%, to be precise) have a reading level below that of the most readable pamphlet. These patients will need help to understand the information provided in the cancer pamphlets. Notice that this conclusion follows from considering the distributions as a whole, not simply measures of center or variability, and that the graph contrasts those distributions more immediately than the frequency tables.
https://assessments.lumenlearning.com/assessments/2741
Statistical Significance
Even when we find patterns in data, often there is still uncertainty in various aspects of the data. For example, there may be potential for measurement errors (even your own body temperature can fluctuate by almost 1°F over the course of the day). Or we may only have a “snapshot” of observations from a more long-term process or only a small subset of individuals from the population of interest. In such cases, how can we determine whether patterns we see in our small set of data is convincing evidence of a systematic phenomenon in the larger process or population? Let's take a look at another example.
Example 2: In a study reported in the November 2007 issue of Nature, researchers investigated whether pre-verbal infants take into account an individual’s actions toward others in evaluating that individual as appealing or aversive (Hamlin, Wynn, & Bloom, 2007). In one component of the study, 10-month-old infants were shown a “climber” character (a piece of wood with “googly” eyes glued onto it) that could not make it up a hill in two tries. Then the infants were shown two scenarios for the climber’s next try, one where the climber was pushed to the top of the hill by another character (“helper”), and one where the climber was pushed back down the hill by another character (“hinderer”). The infant was alternately shown these two scenarios several times. Then the infant was presented with two pieces of wood (representing the helper and the hinderer characters) and asked to pick one to play with.
The researchers found that of the 16 infants who made a clear choice, 14 chose to play with the helper toy. One possible explanation for this clear majority result is that the helping behavior of the one toy increases the infants’ likelihood of choosing that toy. But are there other possible explanations? What about the color of the toy? Well, prior to collecting the data, the researchers arranged so that each color and shape (red square and blue circle) would be seen by the same number of infants. Or maybe the infants had right-handed tendencies and so picked whichever toy was closer to their right hand?
Well, prior to collecting the data, the researchers arranged it so half the infants saw the helper toy on the right and half on the left. Or, maybe the shapes of these wooden characters (square, triangle, circle) had an effect? Perhaps, but again, the researchers controlled for this by rotating which shape was the helper toy, the hinderer toy, and the climber. When designing experiments, it is important to control for as many variables as might affect the responses as possible. It is beginning to appear that the researchers accounted for all the other plausible explanations. But there is one more important consideration that cannot be controlled—if we did the study again with these 16 infants, they might not make the same choices. In other words, there is some randomness inherent in their selection process.
P-value
Maybe each infant had no genuine preference at all, and it was simply “random luck” that led to 14 infants picking the helper toy. Although this random component cannot be controlled, we can apply a probability model to investigate the pattern of results that would occur in the long run if random chance were the only factor.
If the infants were equally likely to pick between the two toys, then each infant had a 50% chance of picking the helper toy. It’s like each infant tossed a coin, and if it landed heads, the infant picked the helper toy. So if we tossed a coin 16 times, could it land heads 14 times? Sure, it’s possible, but it turns out to be very unlikely. Getting 14 (or more) heads in 16 tosses is about as likely as tossing a coin and getting 9 heads in a row. This probability is referred to as a p-value. The p-value represents the likelihood that experimental results happened by chance. Within psychology, the most common standard for p-values is “p < .05”. What this means is that there is less than a 5% probability that the results happened just by random chance, and therefore a 95% probability that the results reflect a meaningful pattern in human psychology. We call this statistical significance.
https://assessments.lumenlearning.com/assessments/2743
So, in the study above, if we assume that each infant was choosing equally, then the probability that 14 or more out of 16 infants would choose the helper toy is found to be 0.0021. We have only two logical possibilities: either the infants have a genuine preference for the helper toy, or the infants have no preference (50/50), and an outcome that would occur only 2 times in 1,000 iterations happened in this study. Because this p-value of 0.0021 is quite small, we conclude that the study provides very strong evidence that these infants have a genuine preference for the helper toy.
If we compare the p-value to some cut-off value, like 0.05, we see that the p=value is smaller. Because the p-value is smaller than that cut-off value, then we reject the hypothesis that only random chance was at play here. In this case, these researchers would conclude that significantly more than half of the infants in the study chose the helper toy, giving strong evidence of a genuine preference for the toy with the helping behavior.
https://assessments.lumenlearning.com/assessments/2742
Generalizability

One limitation to the study mentioned previously about the babies choosing the "helper" toy is that the conclusion only applies to the 16 infants in the study. We don’t know much about how those 16 infants were selected. Suppose we want to select a subset of individuals (a sample) from a much larger group of individuals (the population) in such a way that conclusions from the sample can be generalized to the larger population. This is the question faced by pollsters every day.
Example 3: The General Social Survey (GSS) is a survey on societal trends conducted every other year in the United States. Based on a sample of about 2,000 adult Americans, researchers make claims about what percentage of the U.S. population consider themselves to be “liberal,” what percentage consider themselves “happy,” what percentage feel “rushed” in their daily lives, and many other issues. The key to making these claims about the larger population of all American adults lies in how the sample is selected. The goal is to select a sample that is representative of the population, and a common way to achieve this goal is to select a random sample that gives every member of the population an equal chance of being selected for the sample. In its simplest form, random sampling involves numbering every member of the population and then using a computer to randomly select the subset to be surveyed. Most polls don’t operate exactly like this, but they do use probability-based sampling methods to select individuals from nationally representative panels.
https://assessments.lumenlearning.com/assessments/2747
In 2004, the GSS reported that 817 of 977 respondents (or 83.6%) indicated that they always or sometimes feel rushed. This is a clear majority, but we again need to consider variation due to random sampling. Fortunately, we can use the same probability model we did in the previous example to investigate the probable size of this error. (Note, we can use the coin-tossing model when the actual population size is much, much larger than the sample size, as then we can still consider the probability to be the same for every individual in the sample.) This probability model predicts that the sample result will be within 3 percentage points of the population value (roughly 1 over the square root of the sample size, the margin of error). A statistician would conclude, with 95% confidence, that between 80.6% and 86.6% of all adult Americans in 2004 would have responded that they sometimes or always feel rushed.
https://assessments.lumenlearning.com/assessments/2748
The key to the margin of error is that when we use a probability sampling method, we can make claims about how often (in the long run, with repeated random sampling) the sample result would fall within a certain distance from the unknown population value by chance (meaning by random sampling variation) alone. Conversely, non-random samples are often suspect to bias, meaning the sampling method systematically over-represents some segments of the population and under-represents others. We also still need to consider other sources of bias, such as individuals not responding honestly. These sources of error are not measured by the margin of error.
Cause and Effect Conclusions
In many research studies, the primary question of interest concerns differences between groups. Then the question becomes how were the groups formed (e.g., selecting people who already drink coffee vs. those who don’t). In some studies, the researchers actively form the groups themselves. But then we have a similar question—could any differences we observe in the groups be an artifact of that group-formation process? Or maybe the difference we observe in the groups is so large that we can discount a “fluke” in the group-formation process as a reasonable explanation for what we find?
Example 4: A psychology study investigated whether people tend to display more creativity when they are thinking about intrinsic (internal) or extrinsic (external) motivations (Ramsey & Schafer, 2002, based on a study by Amabile, 1985). The subjects were 47 people with extensive experience with creative writing. Subjects began by answering survey questions about either intrinsic motivations for writing (such as the pleasure of self-expression) or extrinsic motivations (such as public recognition). Then all subjects were instructed to write a haiku, and those poems were evaluated for creativity by a panel of judges. The researchers conjectured beforehand that subjects who were thinking about intrinsic motivations would display more creativity than subjects who were thinking about extrinsic motivations. The creativity scores from the 47 subjects in this study are displayed in Figure 2.6.5, where higher scores indicate more creativity.
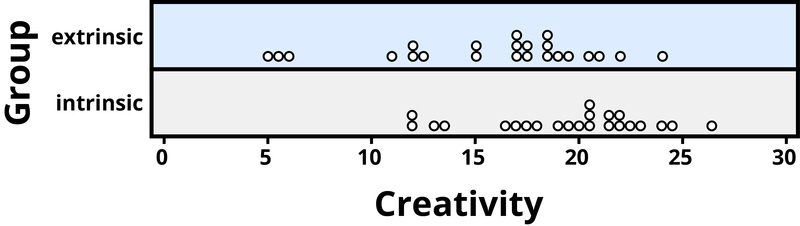
In this example, the key question is whether the type of motivation affects creativity scores. In particular, do subjects who were asked about intrinsic motivations tend to have higher creativity scores than subjects who were asked about extrinsic motivations?
Figure 2.6.5 reveals that both motivation groups saw considerable variability in creativity scores, and these scores have considerable overlap between the groups. In other words, it’s certainly not always the case that those with extrinsic motivations have higher creativity than those with intrinsic motivations, but there may still be a statistical tendency in this direction. (Psychologist Keith Stanovich (2013) refers to people’s difficulties with thinking about such probabilistic tendencies as “the Achilles heel of human cognition.”)
The mean creativity score is 19.88 for the intrinsic group, compared to 15.74 for the extrinsic group, which supports the researchers’ conjecture. Yet comparing only the means of the two groups fails to consider the variability of creativity scores in the groups. We can measure variability with statistics using, for instance, the standard deviation: 5.25 for the extrinsic group and 4.40 for the intrinsic group. The standard deviations tell us that most of the creativity scores are within about 5 points of the mean score in each group. We see that the mean score for the intrinsic group lies within one standard deviation of the mean score for extrinsic group. So, although there is a tendency for the creativity scores to be higher in the intrinsic group, on average, the difference is not extremely large.
We again want to consider possible explanations for this difference. The study only involved individuals with extensive creative writing experience. Although this limits the population to which we can generalize, it does not explain why the mean creativity score was a bit larger for the intrinsic group than for the extrinsic group. Maybe women tend to receive higher creativity scores? Here is where we need to focus on how the individuals were assigned to the motivation groups. If only women were in the intrinsic motivation group and only men in the extrinsic group, then this would present a problem because we wouldn’t know if the intrinsic group did better because of the different type of motivation or because they were women. However, the researchers guarded against such a problem by randomly assigning the individuals to the motivation groups. Like flipping a coin, each individual was just as likely to be assigned to either type of motivation. Why is this helpful? Because this random assignment tends to balance out all the variables related to creativity we can think of, and even those we don’t think of in advance, between the two groups. So we should have a similar male/female split between the two groups; we should have a similar age distribution between the two groups; we should have a similar distribution of educational background between the two groups; and so on. Random assignment should produce groups that are as similar as possible except for the type of motivation, which presumably eliminates all those other variables as possible explanations for the observed tendency for higher scores in the intrinsic group.
But does this always work? No, so by “luck of the draw” the groups may be a little different prior to answering the motivation survey. So then the question is, is it possible that an unlucky random assignment is responsible for the observed difference in creativity scores between the groups? In other words, suppose each individual’s poem was going to get the same creativity score no matter which group they were assigned to, that the type of motivation in no way impacted their score. Then how often would the random-assignment process alone lead to a difference in mean creativity scores as large (or larger) than 19.88 – 15.74 = 4.14 points?
We again want to apply to a probability model to approximate a p-value, but this time the model will be a bit different. Think of writing everyone’s creativity scores on an index card, shuffling up the index cards, and then dealing out 23 to the extrinsic motivation group and 24 to the intrinsic motivation group, and finding the difference in the group means. We (better yet, the computer) can repeat this process over and over to see how often, when the scores don’t change, random assignment leads to a difference in means at least as large as 4.41. Figure 2.6.6 shows the results from 1,000 such hypothetical random assignments for these scores.
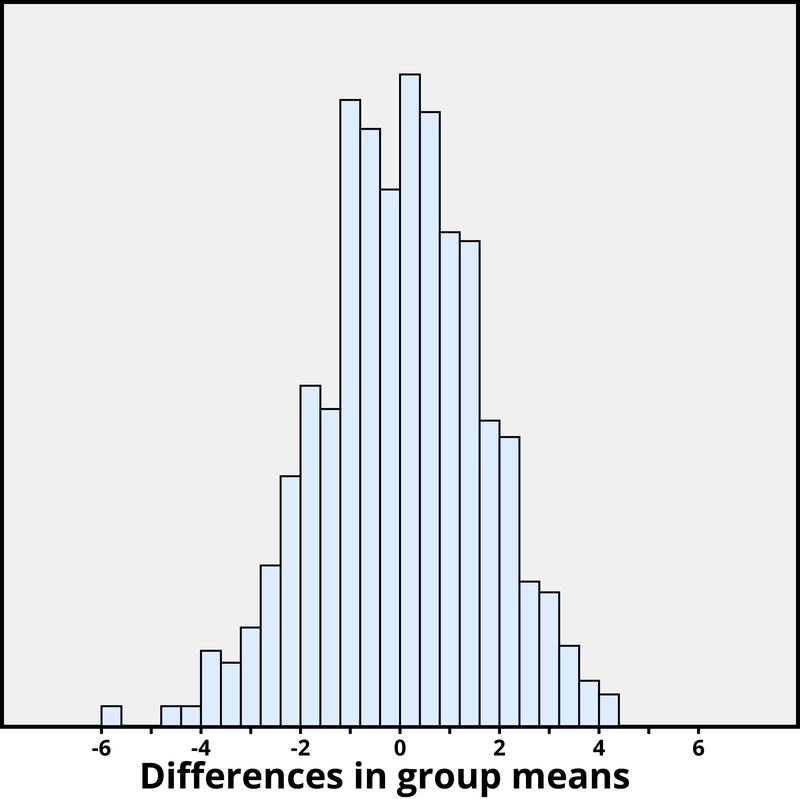
Only 2 of the 1,000 simulated random assignments produced a difference in group means of 4.41 or larger. In other words, the approximate p-value is 2/1000 = 0.002. This small p-value indicates that it would be very surprising for the random assignment process alone to produce such a large difference in group means. Therefore, as with Example 4, we have strong evidence that focusing on intrinsic motivations tends to increase creativity scores, as compared to thinking about extrinsic motivations.
Notice that the previous statement implies a cause-and-effect relationship between motivation and creativity score; is such a strong conclusion justified? Yes, because of the random assignment used in the study. That should have balanced out any other variables between the two groups, so now that the small p-value convinces us that the higher mean in the intrinsic group wasn’t just a coincidence, the only reasonable explanation left is the difference in the type of motivation. Can we generalize this conclusion to everyone? Not necessarily—we could cautiously generalize this conclusion to individuals with extensive experience in creative writing similar to the individuals in this study, but we would still want to know more about how these individuals were selected to participate.
https://assessments.lumenlearning.com/assessments/2709
Conclusion
Statistical thinking involves the careful design of a study to collect meaningful data to answer a focused research question, detailed analysis of patterns in the data, and drawing conclusions that go beyond the observed data. Random sampling is paramount to generalizing results from our sample to a larger population, and random assignment is key to drawing cause-and-effect conclusions. With both kinds of randomness, probability models help us assess how much random variation we can expect in our results, in order to determine whether our results could happen by chance alone and to estimate a margin of error.
So where does this leave us with regard to the coffee study mentioned previously (the Freedman, Park, Abnet, Hollenbeck, & Sinha, 2012 found that men who drank at least six cups of coffee a day had a 10% lower chance of dying (women 15% lower) than those who drank none)? We can answer many of the questions:
- This was a 14-year study conducted by researchers at the National Cancer Institute.
- The results were published in the June issue of the New England Journal of Medicine, a respected, peer-reviewed journal.
- The study reviewed coffee habits of more than 402,000 people ages 50 to 71 from six states and two metropolitan areas. Those with cancer, heart disease, and stroke were excluded at the start of the study. Coffee consumption was assessed once at the start of the study.
- About 52,000 people died during the course of the study.
- People who drank between two and five cups of coffee daily showed a lower risk as well, but the amount of reduction increased for those drinking six or more cups.
- The sample sizes were fairly large and so the p-values are quite small, even though percent reduction in risk was not extremely large (dropping from a 12% chance to about 10%–11%).
- Whether coffee was caffeinated or decaffeinated did not appear to affect the results.
- This was an observational study, so no cause-and-effect conclusions can be drawn between coffee drinking and increased longevity, contrary to the impression conveyed by many news headlines about this study. In particular, it’s possible that those with chronic diseases don’t tend to drink coffee.
This study needs to be reviewed in the larger context of similar studies and consistency of results across studies, with the constant caution that this was not a randomized experiment. Whereas a statistical analysis can still “adjust” for other potential confounding variables, we are not yet convinced that researchers have identified them all or completely isolated why this decrease in death risk is evident. Researchers can now take the findings of this study and develop more focused studies that address new questions.
Learn More
Explore these outside resources to learn more about applied statistics:
- Video about p-values: P-Value Extravaganza
- Interactive web applets for teaching and learning statistics
- Inter-university Consortium for Political and Social Research where you can find and analyze data.
- The Consortium for the Advancement of Undergraduate Statistics
Principles of Physical Development
Growth is influenced by the two major trends, cephalocaudal development (from head to tow, where your brain is developed first ) and proximodistal development (from the midline outward where your organs will be more developed than extremities such as your limbs and arms). In early childhood, the average child grows 2½ inches and between 5 to 7 pounds a year. Girls are slightly smaller and lighter than boys.

Hormonal influence
Hormones play a vital role in the body’s physical development. They are chemical messengers released by the endocrine system and sent throughout the body to regulate various physiological processes and behaviors. In addition to influencing physical development, hormones also affect cognitive and socioemotional growth.
During early childhood, two hormones are especially important for physical growth. The first is Human Growth Hormone (HGH), which supports growth in nearly all parts of the body except the central nervous system (CNS). Growth in the CNS is primarily influenced by the Thyroid Stimulating Hormone (TSH). Together, these hormones help regulate the overall growth process during early developmental stages.
During puberty, the release of sex hormones—primarily estrogen in females and testosterone in males—plays a central role in the development of sexual organs and secondary sex characteristics. We will explore these changes in more detail later in this module.
Video 3.1.1. Explaining the two systems that is responsible for producing and releasing hormone in our body.
Anderson, N. E. (2014). A racial/ethnic comparison of teen sexual attitudes and behavior. Health behavior and policy review, 1(1), 16-27.
Andrews, K. M., & Moore, K. A. (2011). Second Chance Homes: A resource for teen mothers. Children, 21, 6.
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American psychologist, 55(5), 469.
Barnett, N. P., Smoll, F. L., & Smith, R. E. (1992). Effects of enhancing coach-athlete relationships on youth sport attrition. The sport psychologist, 6(2), 111-127.
Flannery, D. J., Rowe, D. C., & Gulley, B. L. (1993). Impact of pubertal status, timing, and age on adolescent sexual experience and delinquency. Journal of Adolescent Research, 8(1), 21-40.
Fraser-Thomas, J. L., Côté, J., & Deakin, J. (2005). Youth sport programs: An avenue to foster positive youth development. Physical education & sport pedagogy, 10(1), 19-40.
Fryar, C. D., Carroll, M. D., & Ogden, C. L. (2014). Prevalence of overweight and obesity among children and adolescents: United States, 1963–1965 through 2011–2012. Atlanta, GA: National Center for Health Statistics.
Ge, X., Conger, R. D., & Elder Jr, G. H. (2001). Pubertal transition, stressful life events, and the emergence of gender differences in adolescent depressive symptoms. Developmental psychology, 37(3), 404.
Graber, J. A., Lewinsohn, P. M., Seeley, J. R., & Brooks-Gunn, J. (1997). Is psychopathology associated with the timing of pubertal development?. Journal of the American Academy of Child & Adolescent Psychiatry, 36(12), 1768-1776.
Graber, J. A. (2013). Pubertal timing and the development of psychopathology in adolescence and beyond. Hormones and behavior, 64(2), 262-269.
Harding, D. J. (2003). Counterfactual models of neighborhood effects: The effect of neighborhood poverty on dropping out and teenage pregnancy. American journal of Sociology, 109(3), 676-719.
Kaltiala-Heino, R., Rimpel, M., Rissanen, A., & Rantanen, P. (2001). Early puberty and early sexual activity are associated with bulimic-type eating pathology in middle adolescence. Journal of Adolescent Health, 28(4), 346-352.
Kristof, N. (2011). What about American girls sold on the streets?. New York Times, 23.
Kost, K., Henshaw, S., & Carlin, L. (2010). US teenage pregnancies, births and abortions: National and state trends and trends by race and ethnicity. New York: Guttmacher Institute.
Martinez, G., Copen, C. E., & Abma, J. C. (2011). Teenagers in the United States: sexual activity, contraceptive use, and childbearing, 2006-2010 national survey of family growth.
McGuine, T. A. (2016). The Association of Sport Specialization and the History of Lower Extremity Injury in High School Athletes.: 3062 Board# 127 June 3, 3: 30 PM-5: 00 PM. Medicine & Science in Sports & Exercise, 48(5S), 866.
Mendle, J., Moore, S. R., Briley, D. A., & Harden, K. P. (2016). Puberty, socioeconomic status, and depression in girls: Evidence for gene× environment interactions. Clinical psychological science, 4(1), 3-16.
Perper, K., & Manlove, J. (2009). Estimated Percentage of Females Who Will Become Teen Mothers: Differences across States. Research Brief. Publication# 2009-09. Child Trends.
Pollack, W. S., & Shuster, T. (2001). Real Boys' Voices: Boys Speak out about Drugs, Sex, Violence, Bullying, Sports, Girls, School, Parents, and So Much More. Penguin.
Rudolph, K. D., Troop-Gordon, W., Lambert, S. F., & Natsuaki, M. N. (2014). Long-term consequences of pubertal timing for youth depression: Identifying personal and contextual pathways of risk. Development and psychopathology, 26(4pt2), 1423-1444.
Sabo, D., & Veliz, P. (2008). Go out and play: Youth sports in America. Women's Sports Foundation.
Steinberg, L. (2013). Adolescence, 10th Edn New York. NY: McGraw-Hill Education.[Google Scholar].
Striegel-Moore, R. H., & Cachelin, F. M. (1999). Body image concerns and disordered eating in adolescent girls: Risk and protective factors.
Tolman, D. L., & McClelland, S. I. (2011). Normative sexuality development in adolescence: A decade in review, 2000–2009. Journal of research on adolescence, 21(1), 242-255.
Van de Bongardt, D., Yu, R., Deković, M., & Meeus, W. H. (2015). Romantic relationships and sexuality in adolescence and young adulthood: The role of parents, peers, and partners. European journal of developmental psychology, 12(5), 497-515.
Wildsmith, E., Schelar, E., Peterson, K., & Manlove, J. (2010). Sexually transmitted diseases among young adults: Prevalence, perceived risk, and risk-taking behaviors. Child Trends Research Brief, 10, 1-8.
Weintraub, D., Chiang, C., Kim, H. M., Wilkinson, J., Marras, C., Stanislawski, B., ... & Kales, H. C. (2016). Association of antipsychotic use with mortality risk in patients with Parkinson disease. JAMA neurology, 73(5), 535-541.
Children grow and develop at a rapid pace. The development of both gross and fine motor skills helps a child to develop and allow them to participate in more activities. Motor development occurs in an orderly sequence as infants move from reflexive reactions (e.g., sucking and rooting) to more advanced motor functioning. As motor skills develop, there are certain developmental milestones that young children should achieve. For each milestone there is an average age, as well as a range of ages in which the milestone should be reached.
Fine motor skills focus on the muscles in our fingers, toes, and eyes, and enable coordination of small actions (e.g., grasping a toy, writing with a pencil, and using a spoon). In middle childhood, fine motor skills are also being refined in activities such as pouring water into a container, drawing, coloring, and using scissors. Some children’s songs promote fine motor skills as well (have you ever heard of the song “itsy, bitsy, spider”?). Mastering the fine art of cutting one’s own fingernails or tying shoes will take a lot of practice and maturation.
Motor skills continue to develop during middle childhood, especially as children enter the school system and gain more opportunities to practice writing. For example, by the age of six, most children can write the alphabet, their name, and the numbers 1 through 10. However, it is not uncommon for them to use their whole arm while writing, which often results in large and uneven letters. As their fine motor skills continue to improve, their handwriting becomes more controlled and legible.
Gross motor skills focus on large muscle groups that control our head, torso, arms and legs and involve larger movements (e.g., balancing, running, and jumping). These skills begin to develop first. Examples include moving to bring the chin up when lying on the stomach, moving the chest up, and rocking back and forth on hands and knees. As children enter primary school, they have more opportunities to participate in organized sports, which contributes to the development of their gross motor skills. In general, gross motor skills improve in four major areas during middle childhood: flexibility, balance, agility, and force.

Exercise and Sports
Middle childhood seems to be a great time to introduce children to organized sports, and in fact, many parents do. Nearly 3 million children play soccer in the United States (United States Youth Soccer, 2012). This activity promises to help children build social skills, improve athletically, and learn a sense of competition. However, it has been suggested that the emphasis on competition and athletic abilities can be counterproductive and lead children to grow tired of the game and want to quit. In many respects, it appears that children’s activities are no longer children’s activities once adults become involved and approach the games as adults rather than children. The U. S. Soccer Federation recently advised coaches to reduce the amount of drilling engaged in during practice and to allow children to play more freely and to choose their own positions. The hope is that this will build on their love of the game and foster their natural talents.
Sports are important for children. Children’s participation in sports has been linked to:
- Higher levels of satisfaction with family and overall quality of life in children
- Improved physical and emotional development
- Better academic performance
CDC ( U.S. Department of Health and Human Services, 2018) recommends that children and adolescents between the age of 6 to 17 years old to have 60 minutes or more of moderate-to-vigorous intensity physical activity each day, including:
- Aerobic activity: Most of the daily 60 minutes or more should include activities such as walking, running, or anything that makes their hearts beat faster. At least 3 days a week should include vigorous-intensity activities.
- Muscle-strengthening: Includes activities like climbing or doing push-ups, at least 3 days a week.
- Bone-strengthening: Includes activities such as jumping or running, at least 3 days a week.
Yet, a study on children’s sports in the United States (Sabo & Veliz, 2008) has found that gender, poverty, location, ethnicity, and disability can limit opportunities to engage in sports. Girls were more likely to have never participated in any type of sport (see Figure 3.2.1). They also found that fathers may not be providing their daughters as much support as they do their sons.
While boys rated their fathers as their biggest mentor who taught them the most about sports, girls rated coaches, and physical education teachers as their key mentors. Sabo and Veliz also found that children in suburban neighborhoods had much higher participation in sports than boys and girls living in rural or urban centers. In addition, Caucasian girls and boys participated in organized sports at higher rates than minority children (see Figure 3.2.2).

Figure 3.2.1.Participation in organized sports (%) by gender.

Figure 3.2.2. Participation in organized sports (%) by race and ethnicity.
Finally, Sabo and Veliz asked children who had dropped out of organized sports why they left. For both girls and boys, the number one answer was that it was no longer any fun (see Table 4.4.1). According to the Sports Policy and Research Collaborative (SPARC) (2013), almost 1 in 3 children drop out of organized sports, and while there are many factors involved in the decisions to drop out, one suggestion has been the lack of training that coaches of children’s sports receive may be contributing to this attrition (Barnett, Smoll & Smith, 1992). Several studies have found that when coaches receive proper training, the drop-out rate is about 5% instead of the usual 30% (Fraser-Thomas, Côté, & Deakin, 2005; SPARC, 2013).
Table 3.2.1. Top reasons dropped out or stopped playing organized sports by gender

Welcome to the World of E-Sports
The recent SPARC (2016) report on the “State of Play” in the United States highlights a disturbing trend. One in four children between the ages of 5 and 16 rate playing computer games with their friends as a form of exercise. In addition, e-sports, which as SPARC writes, is about as much a sport as poker, involves children watching other children play video games. over half of males, and about 20% of females, aged 12-19, say they are fans of e-sports.
Since 2008 there has also been a downward trend in the number of sports children are engaged in, despite a body of research evidence that suggests that specializing in only one activity can increase the chances of injury while playing multiple sports is protective (SPARC, 2016). A University of Wisconsin study found that 49% of athletes who specialized in a sport experienced an injury compared with 23% of those who played multiple sports (McGuine, 2016).
Physical Education
For many children, physical education in school is a key component in introducing children to sports. After years of schools cutting back on physical education programs, there has been a turnaround, prompted by concerns over childhood obesity and related health issues. Despite these changes, currently, only the state of Oregon and the District of Columbia meet PE guidelines of a minimum of 150 minutes per week of physical activity in elementary school and 225 minutes in middle school (SPARC, 2016).
Barnett, N. P., Smoll, F. L., & Smith, R. E. (1992). Effects of enhancing coach-athlete relationships on youth sport attrition. The sport psychologist, 6(2), 111-127.
Fraser-Thomas, J. L., Côté, J., & Deakin, J. (2005). Youth sport programs: An avenue to foster positive youth development. Physical education & sport pedagogy, 10(1), 19-40.
McGuine, T. A. (2016). The Association of Sport Specialization and the History of Lower Extremity Injury in High School Athletes.: 3062 Board# 127 June 3, 3: 30 PM-5: 00 PM. Medicine & Science in Sports & Exercise, 48(5S), 866.
Sabo, D., & Veliz, P. (2008). Go out and play: Youth sports in America. Women's Sports Foundation.
Anderson, N. E. (2014). A racial/ethnic comparison of teen sexual attitudes and behavior. Health behavior and policy review, 1(1), 16-27.
Andrews, K. M., & Moore, K. A. (2011). Second Chance Homes: A resource for teen mothers. Children, 21, 6.
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American psychologist, 55(5), 469.
Barnett, N. P., Smoll, F. L., & Smith, R. E. (1992). Effects of enhancing coach-athlete relationships on youth sport attrition. The sport psychologist, 6(2), 111-127.
Flannery, D. J., Rowe, D. C., & Gulley, B. L. (1993). Impact of pubertal status, timing, and age on adolescent sexual experience and delinquency. Journal of Adolescent Research, 8(1), 21-40.
Fraser-Thomas, J. L., Côté, J., & Deakin, J. (2005). Youth sport programs: An avenue to foster positive youth development. Physical education & sport pedagogy, 10(1), 19-40.
Fryar, C. D., Carroll, M. D., & Ogden, C. L. (2014). Prevalence of overweight and obesity among children and adolescents: United States, 1963–1965 through 2011–2012. Atlanta, GA: National Center for Health Statistics.
Ge, X., Conger, R. D., & Elder Jr, G. H. (2001). Pubertal transition, stressful life events, and the emergence of gender differences in adolescent depressive symptoms. Developmental psychology, 37(3), 404.
Graber, J. A., Lewinsohn, P. M., Seeley, J. R., & Brooks-Gunn, J. (1997). Is psychopathology associated with the timing of pubertal development?. Journal of the American Academy of Child & Adolescent Psychiatry, 36(12), 1768-1776.
Graber, J. A. (2013). Pubertal timing and the development of psychopathology in adolescence and beyond. Hormones and behavior, 64(2), 262-269.
Harding, D. J. (2003). Counterfactual models of neighborhood effects: The effect of neighborhood poverty on dropping out and teenage pregnancy. American journal of Sociology, 109(3), 676-719.
Kaltiala-Heino, R., Rimpel, M., Rissanen, A., & Rantanen, P. (2001). Early puberty and early sexual activity are associated with bulimic-type eating pathology in middle adolescence. Journal of Adolescent Health, 28(4), 346-352.
Kristof, N. (2011). What about American girls sold on the streets?. New York Times, 23.
Kost, K., Henshaw, S., & Carlin, L. (2010). US teenage pregnancies, births and abortions: National and state trends and trends by race and ethnicity. New York: Guttmacher Institute.
Martinez, G., Copen, C. E., & Abma, J. C. (2011). Teenagers in the United States: sexual activity, contraceptive use, and childbearing, 2006-2010 national survey of family growth.
McGuine, T. A. (2016). The Association of Sport Specialization and the History of Lower Extremity Injury in High School Athletes.: 3062 Board# 127 June 3, 3: 30 PM-5: 00 PM. Medicine & Science in Sports & Exercise, 48(5S), 866.
Mendle, J., Moore, S. R., Briley, D. A., & Harden, K. P. (2016). Puberty, socioeconomic status, and depression in girls: Evidence for gene× environment interactions. Clinical psychological science, 4(1), 3-16.
Perper, K., & Manlove, J. (2009). Estimated Percentage of Females Who Will Become Teen Mothers: Differences across States. Research Brief. Publication# 2009-09. Child Trends.
Pollack, W. S., & Shuster, T. (2001). Real Boys' Voices: Boys Speak out about Drugs, Sex, Violence, Bullying, Sports, Girls, School, Parents, and So Much More. Penguin.
Rudolph, K. D., Troop-Gordon, W., Lambert, S. F., & Natsuaki, M. N. (2014). Long-term consequences of pubertal timing for youth depression: Identifying personal and contextual pathways of risk. Development and psychopathology, 26(4pt2), 1423-1444.
Sabo, D., & Veliz, P. (2008). Go out and play: Youth sports in America. Women's Sports Foundation.
Steinberg, L. (2013). Adolescence, 10th Edn New York. NY: McGraw-Hill Education.[Google Scholar].
Striegel-Moore, R. H., & Cachelin, F. M. (1999). Body image concerns and disordered eating in adolescent girls: Risk and protective factors.
Tolman, D. L., & McClelland, S. I. (2011). Normative sexuality development in adolescence: A decade in review, 2000–2009. Journal of research on adolescence, 21(1), 242-255.
Van de Bongardt, D., Yu, R., Deković, M., & Meeus, W. H. (2015). Romantic relationships and sexuality in adolescence and young adulthood: The role of parents, peers, and partners. European journal of developmental psychology, 12(5), 497-515.
Wildsmith, E., Schelar, E., Peterson, K., & Manlove, J. (2010). Sexually transmitted diseases among young adults: Prevalence, perceived risk, and risk-taking behaviors. Child Trends Research Brief, 10, 1-8.
Weintraub, D., Chiang, C., Kim, H. M., Wilkinson, J., Marras, C., Stanislawski, B., ... & Kales, H. C. (2016). Association of antipsychotic use with mortality risk in patients with Parkinson disease. JAMA neurology, 73(5), 535-541.
Puberty is the period of rapid growth and sexual development that begins in adolescence and starts at some point between ages 8 and 14. While the sequence of physical changes in puberty is predictable, the onset and pace of puberty vary widely. Every person’s individual timetable for puberty is different and is primarily influenced by heredity; however, environmental factors—such as diet and exercise—also exert some influence.
Adolescence has evolved historically, with evidence indicating that this stage is lengthening as individuals start puberty earlier and transition to adulthood later than in the past. Puberty today begins, on average, at age 10–11 years for girls and 11–12 years for boys. This average age of onset has decreased gradually over time since the 19th century by 3–4 months per decade, which has been attributed to a range of factors including better nutrition, obesity, increased father absence, and other environmental factors (Steinberg, 2013). Completion of formal education, financial independence from parents, marriage, and parenthood have all been markers of the end of adolescence and beginning of adulthood, and all of these transitions happen, on average, later now than in the past. In fact, the prolonging of adolescence has prompted the introduction of a new developmental period called emerging adulthood that captures these developmental changes out of adolescence and into adulthood, occurring approximately from ages 18 to 29 (Arnett, 2000).


Figure 4.2.1. Major physical changes during puberty.
Hormonal Changes
Puberty involves distinctive physiological changes in an individual’s height, weight, body composition, and circulatory and respiratory systems, and during this time, both the adrenal glands and sex glands mature. These changes are primarily influenced by hormonal activity. Many hormones contribute to the beginning of puberty, but most notably, a significant rush of estrogen for girls and testosterone for boys. Hormones play an organizational role (priming the body to behave in a certain way once puberty begins) and an activational role (triggering certain behavioral and physical changes). During puberty, the adolescent’s hormonal balance shifts sharply towards an adult state; the process is triggered by the pituitary gland, which secretes a surge of hormonal agents into the bloodstream and initiates a chain reaction.
Puberty occurs over two distinct phases, and the first phase, adrenarche, begins at 6 to 8 years of age and involves increased production of adrenal androgens that contribute to a number of pubertal changes—such as skeletal growth. The second phase of puberty, gonadarche, begins several years later and involves increased production of hormones governing physical and sexual maturation.
Sexual Maturation
During puberty, primary and secondary sex characteristics develop and mature. Primary sex characteristics are organs specifically needed for reproduction—the uterus and ovaries in females and testes in males. Secondary sex characteristics are physical signs of sexual maturation that do not directly involve sex organs, such as the development of breasts and hips in girls, and growth of facial hair and a deepened voice in boys. Both sexes experience the development of pubic and underarm hair, as well as increased development of sweat glands.
The male and female gonads are activated by the surge of the hormones discussed earlier, which puts them into a state of rapid growth and development. The testes primarily release testosterone, and the ovaries release estrogen; the production of these hormones increases gradually until sexual maturation is met.
For girls, observable changes begin with nipple growth and pubic hair. Then the body increases in height while fat forms, particularly on the breasts and hips. The first menstrual period (menarche) is followed by more growth, which is usually completed by four years after the first menstrual period began. Girls experience menarche usually around 12–13 years old. For boys, the usual sequence is growth of the testes, initial pubic-hair growth, growth of the penis, first ejaculation of seminal fluid (spermarche), appearance of facial hair, a peak growth spurt, deepening of the voice, and final pubic-hair growth. (Herman-Giddens et al., 2012). Boys experience spermarche, the first ejaculation, around 13–14 years old.
Physical Growth: The Growth Spurt
During puberty, both sexes experience a rapid increase in height and weight (referred to as a growth spurt) over about 2-3 years resulting from the simultaneous release of growth hormones, thyroid hormones, and androgens. Males experience their growth spurt about two years later than females. For girls, the growth spurt begins between 8 and 13 years old (average 10-11), with adult height reached between 10 and 16 years old. Boys begin their growth spurt slightly later, usually between 10 and 16 years old (average 12-13), and reach their adult height between 13 and 17 years old. Both nature (i.e., genes) and nurture (e.g., nutrition, medications, and medical conditions) can influence both height and weight.
Before puberty, there are nearly no differences between males and females in the distribution of fat and muscle. During puberty, males grow muscle much faster than females, and females experience a higher increase in body fat, and bones become harder and more brittle. An adolescent’s heart and lungs increase in both size and capacity during puberty; these changes contribute to increased strength and tolerance for exercise.
Reactions Toward Puberty and Physical Development
The accelerated growth in different body parts happens at different times, but for all adolescents, it has a fairly regular sequence. The first places to grow are the extremities (head, hands, and feet), followed by the arms and legs, and later the torso and shoulders. This non-uniform growth is one reason why an adolescent body may seem out of proportion. Additionally, because rates of physical development vary widely among teenagers, puberty can be a source of pride or embarrassment.
Most adolescents want nothing more than to fit in and not be distinguished from their peers in any way, shape, or form (Mendle et al., 2016). So when a child develops earlier or later than his or her peers, there can be long-lasting effects on mental health. Simply put, beginning puberty earlier than peers presents significant challenges, particularly for girls. The picture for early-developing boys isn’t as clear, but evidence suggests that they, too, eventually might suffer ill effects from maturing ahead of their peers. The biggest challenges for boys, however, seem to be more related to late development.
Early maturing boys tend to be stronger, taller, and more athletic than their later maturing peers. They are usually more popular, confident, and independent, but they are also at a greater risk for substance abuse and early sexual activity (Flannery, Rowe, & Gulley, 1993; Kaltiala-Heino, Rimpela, Rissanen, & Rantanen, 2001). Additionally, more recent research found that while early-maturing boys initially had lower levels of depression than later-maturing boys, over time, they showed signs of increased anxiety, negative self-image, and interpersonal stress. (Rudolph, Troop-Gordon, Lambert, & Natsuaki, 2014).
Early maturing girls may be teased or overtly admired, which can cause them to feel self-conscious about their developing bodies. These girls are at increased risk of a range of psychosocial problems, including depression, substance use, and early sexual behavior (Graber, 2013).These girls are also at a higher risk for eating disorders, which we will discuss in more detail later in this module (Ge, Conger, & Elder, 2001; Graber, Lewinsohn, Seeley, & Brooks-Gunn, 1997; Striegel-Moore & Cachelin, 1999).
Late maturing boys and girls (i.e., they develop more slowly than their peers) may feel self-conscious about their lack of physical development. Negative feelings are particularly a problem for late maturing boys, who are at a higher risk for depression and conflict with parents (Graber et al., 1997) and more likely to be bullied (Pollack & Shuster, 2000).
https://youtu.be/DWKWjpVsGng
Video 3.3.1. Development in Adolescence provides an overview of physical changes during adolescence and psychosocial impacts.
https://assessments.lumenlearning.com/assessments/16609
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American psychologist, 55(5), 469.
Barnett, N. P., Smoll, F. L., & Smith, R. E. (1992). Effects of enhancing coach-athlete relationships on youth sport attrition. The sport psychologist, 6(2), 111-127.
Flannery, D. J., Rowe, D. C., & Gulley, B. L. (1993). Impact of pubertal status, timing, and age on adolescent sexual experience and delinquency. Journal of Adolescent Research, 8(1), 21-40.
Fraser-Thomas, J. L., Côté, J., & Deakin, J. (2005). Youth sport programs: An avenue to foster positive youth development. Physical education & sport pedagogy, 10(1), 19-40.
Ge, X., Conger, R. D., & Elder Jr, G. H. (2001). Pubertal transition, stressful life events, and the emergence of gender differences in adolescent depressive symptoms. Developmental psychology, 37(3), 404.
Graber, J. A., Lewinsohn, P. M., Seeley, J. R., & Brooks-Gunn, J. (1997). Is psychopathology associated with the timing of pubertal development?. Journal of the American Academy of Child & Adolescent Psychiatry, 36(12), 1768-1776.
Graber, J. A. (2013). Pubertal timing and the development of psychopathology in adolescence and beyond. Hormones and behavior, 64(2), 262-269.
Kaltiala-Heino, R., Rimpel, M., Rissanen, A., & Rantanen, P. (2001). Early puberty and early sexual activity are associated with bulimic-type eating pathology in middle adolescence. Journal of Adolescent Health, 28(4), 346-352.
McGuine, T. A. (2016). The Association of Sport Specialization and the History of Lower Extremity Injury in High School Athletes.: 3062 Board# 127 June 3, 3: 30 PM-5: 00 PM. Medicine & Science in Sports & Exercise, 48(5S), 866.
Mendle, J., Moore, S. R., Briley, D. A., & Harden, K. P. (2016). Puberty, socioeconomic status, and depression in girls: Evidence for gene× environment interactions. Clinical psychological science, 4(1), 3-16.
Pollack, W. S., & Shuster, T. (2001). Real Boys' Voices: Boys Speak out about Drugs, Sex, Violence, Bullying, Sports, Girls, School, Parents, and So Much More. Penguin.
Rudolph, K. D., Troop-Gordon, W., Lambert, S. F., & Natsuaki, M. N. (2014). Long-term consequences of pubertal timing for youth depression: Identifying personal and contextual pathways of risk. Development and psychopathology, 26(4pt2), 1423-1444.
Sabo, D., & Veliz, P. (2008). Go out and play: Youth sports in America. Women's Sports Foundation.
Steinberg, L. (2013). Adolescence, 10th Edn New York. NY: McGraw-Hill Education.[Google Scholar].
Striegel-Moore, R. H., & Cachelin, F. M. (1999). Body image concerns and disordered eating in adolescent girls: Risk and protective factors.
Nutrition
Adequate nutrition is necessary for optimal growth and development. Dietary choices and habits established during middle childhood and adolescence greatly influence future health, yet many studies report that children consume few fruits and vegetables and are not receiving the calcium, iron, vitamins, or minerals necessary for healthy development.
One of the reasons for poor nutrition is anxiety about body image, which is a person’s idea of how his or her body looks. Children as young as 6 years old are worrying about their size, body image dissatisfaction generally increases as children get older. The way children feel about their bodies can affect the way they feel about themselves as a whole. Few adolescents welcome their sudden weight increase, so they may adjust their eating habits to lose weight. Adding to the rapid physical changes, they are simultaneously bombarded by messages, and sometimes teasing, related to body image, appearance, attractiveness, weight, and eating that they encounter in the media, at home, and from their friends/peers (both in-person and via social media).
Much research has been conducted on the psychological ramifications of body image on adolescents. Modern-day teenagers are exposed to more media on a daily basis than any generation before them. Recent studies have indicated that the average teenager watches roughly 1500 hours of television per year, and 70% use social media multiple times a day. As such, adolescents are exposed to many representations of ideal, societal beauty. The concept of a person being unhappy with their own image or appearance has been defined as “body dissatisfaction.” In teenagers, body dissatisfaction is often associated with body mass, low self-esteem, and atypical eating patterns. Scholars continue to debate the effects of media on body dissatisfaction in teens. What we do know is that two-thirds of U.S. high school girls are trying to lose weight, and one-third think they are overweight, while only one-sixth are actually overweight (MMWR, June 10, 2016).
Obesity
Although at the peak of physical health, a concern for early adults is the current rate of obesity. Results from the 2015 National Center for Health Statistics indicate that an estimated 70.7% of U.S. adults aged 20 and over are overweight, and 37.9% are obese (CDC, 2015b). Body mass index (BMI), expressed as weight in kilograms divided by height in meters squared (kg/m2), is commonly used to classify overweight (BMI 25.0–29.9), obesity (BMI greater than or equal to 30.0), and extreme obesity (BMI greater than or equal to 40.0). The 2015 statistics show an increase from the 2013-2014 statistics that indicated that an estimated 35.1% were obese, and 6.4% extremely obese (Fryar, Carroll, & Ogden, 2014). In 2003-2004, 32% of American adults were identified as obese. The CDC also indicated that one’s 20s are the prime time to gain weight as the average person gains one to two pounds per year from early adulthood into middle adulthood. The average man in his 20s weighs around 185 pounds and by his 30s, weighs approximately 200 pounds. The average American woman weighs 162 pounds in her 20s and 170 pounds in her 30s.

Figure 3.5.1. Waist circumference.
The American obesity crisis is also reflected worldwide (Wighton, 2016). In 2014, global obesity rates for men were measured at 10.8% and among women 14.9%. This translates to 266 million obese men and 375 million obese women in the world, and more people were identified as obese than underweight. Although obesity is seen throughout the world, more obese men and women live in China and the USA than in any other country. Figure 4.3 illustrates how waist circumference is also used as a measure of obesity. Figure 4.4 demonstrates the percentage of growth for males and females identified as obese between 1960 and 2012.
Causes of Obesity
According to the Centers for Disease Control and Prevention (CDC) (2016), obesity originates from a complex set of contributing factors, including one’s environment, behavior, and genetics. Societal factors include culture, education, parental attitude, food marketing and promotion, the quality of food, and the physical activity environment available. Behaviors leading to obesity include diet, the amount of physical activity, and medication use. Lastly, there does not appear to be a single gene responsible for obesity. Rather, research has identified variants in several genes that may contribute to obesity by increasing hunger and food intake. Another genetic explanation is the mismatch between today’s environment and “energy-thrifty genes” that multiplied in the distant past when food sources were unpredictable. The genes that helped our ancestors survive occasional famines are now being challenged by environments in which food is plentiful all the time. Overall, obesity most likely results from complex interactions among the environment and multiple genes.

Figure 3.5.2. Adult obesity trends Notes: Age-adjusted by the direct method to the year 2000 U.S. Census Bureau estimates using age groups 20–39, 40–59, and 60–74. Pregnant females were excluded. Overweight is body mass index (BMI) of 25 or greater but less 30; obesity is BMI greater than or equal to 30; and extreme obesity is BMI greater than or equal to 40. SOURCE: CDC/NCHS, National Health Examination Survey 1960–1962; and National Health and Nutrition Examination Surveys 1971–1974; 1976–1980; 1988–1994; 1999–2000, 2001–2002, 2003–2004, 2005–2006, 2007–2008, 2009–2010, and 2011–2012.
Family plays a crucial role in shaping children's attitudes toward food. For example, research has shown that daughters of mothers with eating disorders are at higher risk of developing disordered eating behaviors themselves (Ferreira et al., 2021). Parents influence children’s relationship with food in many ways—even as early as the preschool years. For instance, studies have found that pressuring young children to eat healthy foods can actually backfire, leading to poorer eating habits over time (citation needed). These findings highlight the importance of promoting healthy eating through supportive, non-coercive approaches in the family environment.
Obesity Health Consequences
Obesity is considered to be one of the leading causes of death in the United States and worldwide. Additionally, the medical care costs of obesity in the United States were estimated to be $147 billion in 2008. According to the CDC (2016) compared to those with a normal or healthy weight, people who are obese are at increased risk for many serious diseases and health conditions, including:
- All-causes of death (mortality)
- High blood pressure (Hypertension)
- High LDL cholesterol, low HDL cholesterol, or high levels of triglycerides (Dyslipidemia)
- Type 2 diabetes
- Coronary heart disease
- Stroke
- Gallbladder disease
- Osteoarthritis (a breakdown of cartilage and bone within a joint)
- Sleep apnea and breathing problems
- Some cancers (endometrial, breast, colon, kidney, gallbladder, and liver)
- Low quality of life
- Mental illness such as clinical depression, anxiety, and other mental disorders
- Body pain and difficulty with physical functioning
Strategies on establishing a healthy eating pattern
As previously mentioned, parents play a vital role in shaping their children's eating habits. They are also key influencers in encouraging healthy dietary behaviors. However, it is important to avoid using coercive strategies—such as pressuring a child to eat certain foods—as these approaches can backfire and may actually reduce the child’s willingness to eat healthily.
Instead, effective strategies for promoting healthy eating include:
-
Involving children in food-related activities such as grocery shopping, meal planning, and cooking. This increases their interest in food and helps them feel more in control of their choices.
-
Offering a variety of nutritious options and presenting them in an appealing way (e.g., colorful fruits and vegetables arranged in fun shapes).
-
Modeling healthy eating behaviors by consistently making healthy food choices yourself.
By creating a positive and supportive food environment, parents can help foster lifelong healthy eating habits in their children.
Eating Disorders
Dissatisfaction with body image can explain why many teens, mostly girls, eat erratically or ingest diet pills to lose weight and why boys may take steroids to increase their muscle mass. Although eating disorders can occur in children and adults, they frequently appear during the teen years or young adulthood (NIMH, 2019). Eating disorders affect both genders, although rates among women are 2½ times greater than among men. Similar to women who have eating disorders, some men also have a distorted sense of body image, including muscle dysmorphia or an extreme concern with becoming more muscular.
Because of the high mortality rate, researchers are looking into the etiology of the disorder and associated risk factors. Researchers are finding that eating disorders are caused by a complex interaction of genetic, biological, behavioral, psychological, and social factors (NIMH, 2019). Eating disorders appear to run in families, and researchers are working to identify DNA variations that are linked to the increased risk of developing eating disorders. Researchers have also found differences in patterns of brain activity in women with eating disorders in comparison with healthy women. The main criteria for the most common eating disorders: anorexia nervosa, bulimia nervosa, and binge-eating disorder are described in the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition, DSM-5 (American Psychiatric Association, 2013).
https://youtu.be/bD8KCcipGaY
Video 4.4.1. Eating Disorders explains the symptoms of anorexia nervosa, bulimia nervosa, and binge-eating disorder, as well as common treatments.
Anorexia Nervosa
People with anorexia nervosa may see themselves as overweight, even when they are dangerously underweight. People with anorexia nervosa typically weigh themselves repeatedly, severely restrict the amount of food they eat, often exercise excessively, and/or may force themselves to vomit or use laxatives to lose weight. Anorexia nervosa has the highest mortality rate of any mental disorder. While many people with this disorder die from complications associated with starvation, others die of suicide.
Symptoms of anorexia nervosa include:
- Extremely restricted eating
- Extreme thinness (emaciation)
- A relentless pursuit of thinness and unwillingness to maintain a normal or healthy weight
- Intense fear of gaining weight
- Distorted body image, a self-esteem that is heavily influenced by perceptions of body weight and shape, or a denial of the seriousness of low body weight
Other symptoms may develop over time, including:
- Thinning of the bones (osteopenia or osteoporosis)
- Mild anemia and muscle wasting and weakness
- Brittle hair and nails
- Dry and yellowish skin
- Growth of fine hair all over the body (lanugo)
- Severe constipation
- Low blood pressure slowed breathing and pulse
- Damage to the structure and function of the heart
- Brain damage
- Multiorgan failure
- Drop-in internal body temperature, causing a person to feel cold all the time
- Lethargy, sluggishness, or feeling tired all the time
- Infertility
For those suffering from anorexia, health consequences include an abnormally slow heart rate and low blood pressure, which increases the risk of heart failure. Additionally, there is a reduction in bone density (osteoporosis), muscle loss and weakness, severe dehydration, fainting, fatigue, and overall weakness. Anorexia nervosa has the highest mortality rate of any psychiatric disorder. Individuals with this disorder may die from complications associated with starvation, while others die of suicide. In women, suicide is much more common in those with anorexia than with most other mental disorders.
Bulimia Nervosa
People with bulimia nervosa have recurrent and frequent episodes of eating unusually large amounts of food and feeling a lack of control over these episodes. This binge-eating is followed by behavior that compensates for overeating such as forced vomiting, excessive use of laxatives or diuretics, fasting, excessive exercise, or a combination of these behaviors. People with bulimia nervosa may be slightly underweight, normal weight, or overweight.
Symptoms of bulimia nervosa include:
- Chronically inflamed and sore throat
- Swollen salivary glands in the neck and jaw area
- Worn tooth enamel and increasingly sensitive and decaying teeth as a result of exposure to stomach acid
- Acid reflux disorder and other gastrointestinal problems
- Intestinal distress and irritation from laxative abuse
- Severe dehydration from purging of fluids
- Electrolyte imbalance (too low or too high levels of sodium, calcium, potassium, and other minerals) which can lead to stroke or heart attack
The binging and purging cycle of bulimia can affect the digestive system and lead to electrolyte and chemical imbalances that can affect the heart and other major organs. Frequent vomiting can cause inflammation and possible rupture of the esophagus, as well as tooth decay and staining from stomach acids. Lastly, binge eating disorder results in similar health risks to obesity, including high blood pressure, high cholesterol levels, heart disease, Type II diabetes, and gall bladder disease (National Eating Disorders Association, 2016).
Binge-Eating Disorder
People with binge-eating disorder lose control over his or her eating. Unlike bulimia nervosa, periods of binge-eating are not followed by purging, excessive exercise, or fasting. As a result, people with binge-eating disorder often are overweight or obese. Binge-eating disorder is the most common eating disorder in the U.S.
Symptoms of binge-eating disorder include:
- Eating unusually large amounts of food in a specific amount of time, such as a 2-hour period
- Eating even when you're full or not hungry
- Eating fast during binge episodes
- Eating until you're uncomfortably full
- Eating alone or in secret to avoid embarrassment
- Feeling distressed, ashamed, or guilty about your eating
- Frequently dieting, possibly without weight loss
Eating Disorders Treatment
To treat eating disorders, getting adequate nutrition, and stopping inappropriate behaviors, such as purging, are the foundations of treatment. Treatment plans are tailored to individual needs and include medical care, nutritional counseling, medications (such as antidepressants), and individual, group, and/or family psychotherapy (NIMH, 2019). For example, the Maudsley Approach has parents of adolescents with anorexia nervosa be actively involved in their child’s treatment, such as assuming responsibility for feeding their child. To eliminate binge eating and purging behaviors, cognitive behavioral therapy (CBT) assists sufferers by identifying distorted thinking patterns and changing inaccurate beliefs.
Links to Learning
Visit the National Eating Disorders Association to learn more about eating disorders.
Developing sexually is an expected and natural part of growing into adulthood. Healthy sexual development involves more than sexual behavior. It is the combination of physical sexual maturation (puberty, age-appropriate sexual behaviors), the formation of a positive sexual identity, and a sense of sexual well-being (discussed more in-depth later in this module). During adolescence, teens strive to become comfortable with their changing bodies and to make healthy, safe decisions about which sexual activities, if any, they wish to engage in.
Earlier in the physical development section, we discussed primary and secondary sex characteristics. During puberty, every primary sex organ (the ovaries, uterus, penis, and testes) increases dramatically in size and matures in function. During puberty, reproduction becomes possible. Simultaneously, secondary sex characteristics develop. These characteristics are not required for reproduction, but they do signify masculinity and femininity. At birth, boys and girls have similar body shapes, but during puberty, males widen at the shoulders, and females widen at the hips and develop breasts (examples of secondary sex characteristics). Sexual development is impacted by a dynamic mixture of physical and cognitive change, coupled with social expectations. With physical maturation, adolescents may become alternately fascinated with and chagrined by their changing bodies, and often compare themselves to the development they notice in their peers or see in the media. For example, many adolescent girls focus on their breast development, hoping their breasts will conform to an ideal body image.
As sex hormones cause biological changes, they also affect the brain and trigger sexual thoughts. Culture, however, shapes actual sexual behaviors. Emotions regarding sexual experience, like the rest of puberty, are strongly influenced by cultural norms regarding what is expected at what age, with peers being the most influential. Simply put, the most important influence on adolescents’ sexual activity is not their bodies, but their close friends, who have more influence than do sex or ethnic group norms (van de Bongardt et al., 2015).
Sexual interest and interaction are a natural part of adolescence. Sexual fantasy and masturbation episodes increase between the ages of 10 and 13. Masturbation is very ordinary—even young children have been known to engage in this behavior. As the bodies of children mature, powerful sexual feelings begin to develop, and masturbation helps release sexual tension. For adolescents, masturbation is a common way to explore their erotic potential, and this behavior can continue throughout adult life.
https://youtu.be/QZWd-fhmqmQ
Video 3.4.1. "What Happens When?" Child and Adolescent Sexual Development explains major milestones in sexual development throughout childhood and adolescence, as well as how to support kids during these stages.
Sexual Interactions
Many early social interactions tend to be nonsexual—text messaging, phone calls, email—but by the age of 12 or 13, some young people may pair off and begin dating and experimenting with kissing, touching, and other physical contact, such as oral sex. The vast majority of young adolescents are not prepared emotionally or physically for oral sex and sexual intercourse. If adolescents this young do have sex, they are highly vulnerable to sexual and emotional abuse, sexually transmitted infections (STIs), HIV, and early pregnancy. For STI’s in particular, adolescents are slower to recognize symptoms, tell partners, and get medical treatment, which puts them at risk of infertility and even death.
Adolescents ages 14 to 16 understand the consequences of unprotected sex and teen parenthood, if properly taught, but cognitively they may lack the skills to integrate this knowledge into everyday situations or consistently to act responsibly in the heat of the moment. By the age of 17, many adolescents have willingly experienced sexual intercourse. Teens who have early sexual intercourse report strong peer pressure as a reason behind their decision. Some adolescents are just curious about sex and want to experience it.
Becoming a sexually healthy adult is a developmental task of adolescence that requires integrating psychological, physical, cultural, spiritual, societal, and educational factors. It is particularly important to understand the adolescent in terms of his or her physical, emotional, and cognitive stage. Additionally, healthy adult relationships are more likely to develop when adolescent impulses are not shamed or feared. Guidance is certainly needed, but acknowledging that adolescent sexuality development is both normal and positive would allow for more open communication so adolescents can be more receptive to education concerning the risks (Tolman & McClelland, 2011).
Adolescents are receptive to their culture, to the models they see at home, in school, and in the mass media. These observations influence moral reasoning and moral behavior, which we discuss in more detail later in this module. Decisions regarding sexual behavior are influenced by teens’ ability to think and reason, their values, and their educational experience. Helping adolescents recognize all aspects of sexual development encourages them to make informed and healthy decisions about sexual matters.
Teenage Sexual Activity Trends
Teenagers are much more sexually active today than they were before the sexual revolution of the 1960s and 70s. About 43 percent of never-married teens ages 15–19 of both sexes have had sexual intercourse (Martinez et al., 2011); this percentage represents a drop from its highest point, in 1988, of 51 percent for females and of 60 percent for males. About three-fourths of girls in today’s sexually experienced group and 85 percent of boys in this group use contraception, most often a condom, the first time they ever have sex. In their most recent act of sexual intercourse, almost 86 percent of girls and 93 percent of boys used contraception, again most often a condom.
If 43 percent of teens have had sexual intercourse, that means the majority of teens, 57 percent, have never had intercourse. It is interesting to examine their reasons. The table below identifies the main reason given for never having sexual intercourse. The top reason for both sexes is religion and morals, followed by concern about a possible pregnancy and not having found the right person with whom to have sex (Martinez et al., 2011).
Table 3.4.1. Main Reason Given for Never Having Sexual Intercourse, Ages 15–19 (%)
| Females | Males | |
| Against religion or morals | 38 | 31 |
| Don’t want to get (a female) pregnant | 19 | 25 |
| Haven’t found the right person yet | 17 | 21 |
| Don’t want to get an STI | 7 | 10 |
| In a relationship, but waiting for the right time | 7 | 5 |
| Other reason | 12 | 8 |
The Problem of Teenage Pregnancy
Most teenage pregnancies and births are unplanned and are part of a more general problem for all women in their childbearing years. Almost 700,000 unplanned teenage pregnancies occur annually; another 50,000 teenage pregnancies are planned. These 750,000 teenage pregnancies annually result in some 400,000 births (Kost, Henshaw, & Carlin, 2010). Altogether, about 18 percent of women, or one of every six females, become teen mothers, and in several southern and southwestern states, this percentage is as high as 25–30 percent (Perper & Manlove, 2009).
The birth rate for females aged 15–19 in 2009 was 39.1 births per 1,000 females. This rate represented a substantial decline from the early 1990s when the rate reached a peak of almost 60. However, it was still twice as high as Canada’s rate and much higher yet than other Western democracies (Figure 3.4.1).

Figure 3.4.1. Teenage Birth Rates in Selected Western Democracies
Although teenaged pregnancies (and births from these pregnancies) are far from the majority of all pregnancies, unplanned or planned, they pose special problems (American College of Obstetricians and Gynecologists, 2011; Anderson, 2014). On the individual level, pregnant teenagers are more at risk than older pregnant women for high blood pressure and anemia, and they are also more likely to experience early labor, premature birth, and low birth weight. In addition, because teenagers are more likely than adults to have STIs, pregnant teenagers are more likely than older pregnant women to have an STI while they are pregnant, either because they already had an STI when they conceived or because they contract an STI from having sex during pregnancy.
Many pregnant teenagers decide to drop out of school. If they stay in school, they often must deal with the embarrassment of being pregnant, and the physical and emotional difficulties accompanying their teenage pregnancy can affect their school performance. Once the baby is born, child care typically becomes an enormous problem, whether or not the new mother is in school. Because pregnant teenagers disproportionately come from families that are poor or near-poor, they have few financial resources and often have weak social support networks, either before or after the baby is born (Andrews & Moore, 2011).
At the societal level, teenage pregnancy and motherhood are very costly in at least two important respects. First, because pregnancy and childbirth complications are more common among teenagers, their health-care expenses during and after pregnancy and childbirth are often higher than the expenses incurred by older women. Medicaid, the federal government’s national health plan for poor families, often covers much of these expenses, and the premiums that private health insurance companies charge are higher than otherwise because of their expenses when they insure the families of pregnant teenagers.
Second, the children of teenage mothers are at risk for several kinds of behavioral and developmental problems. Teenage parents may be unprepared emotionally or practically to raise a child. Children of teen parents may receive less cognitive stimulation and proper emotional support. In addition, the stress they experience as young parents put them at risk of neglecting or abusing their children. Teenage parents also tend to come from low-income families and continue to live in poverty or near poverty after they become mothers compounds all these problems. For all these reasons, the children of teenage mothers are at greater risk for several kinds of issues. These problems include impaired neurological development, behavioral problems, poor school performance, and chronic health problems.
Reducing Teenage Pregnancy
In an effort to reduce teenage pregnancies, two approaches have been used: (1) Emphasize abstinence, convincing teens to hold off on having sex until adulthood or marriage, and (2) comprehensive sex education, including teaching the effective use of contraception if they do have sex. Most sexual behavior researchers believe that pleas for abstinence, as well as sex education programs that focus solely or almost entirely on abstinence, do not help to reduce teen sex and pregnancy (Ball & Moore, 2008).
Comprehensive sex education is based on the strategy of harm reduction. A harm reduction approach recognizes that because certain types of harmful behavior are inevitable, our society should do its best to minimize the various kinds of harm that these various behaviors generate. In regard to teenage sex and pregnancy, a harm reduction approach has two goals: (1) to help reduce the risk for pregnancy among sexually active teens and (2) to help teenage parents and their children.
To achieve the first goal, parents, sex education classes, family planning clinics, youth development programs, and other parties must continue to emphasize the importance of waiting to have sex but also the need for teenagers to use contraception if they are sexually active. In addition, effective contraception (birth control pills, other hormonal control, and even condoms, which protect against STIs) must be made available for teenagers at little or no cost. Studies indicate that these two contraception strategies do not lead to more teenage sex, and they also indicate that consistent contraceptive use dramatically reduces the risk of teenage pregnancy. As one writer has summarized these studies’ conclusions, “Contraceptives no more cause sex than umbrellas cause rain…When contraception is unavailable, the likely consequences is not less sex, but more pregnancy” (Kristof, 2011, p. A31).
In this regard, a recent report of the Guttmacher Institute called contraception a “proven, cost-effective strategy” (Gold, 2011, p. 7). It added, “Contraception is almost universally accepted as a way to reduce the risk of unintended pregnancy…Contraceptive use reduces the risk of unintended pregnancy significantly, and consistent contraceptive use virtually eliminates it.” The report noted that government-funded family planning agencies prevent 2 million unintended pregnancies annually by providing contraception to 9 million young and low-income women each year. Because most of the women who would have these prevented pregnancies would be eligible for Medicaid, the Medicaid savings from these prevented pregnancies amount to about $7 billion annually. An expansion of family planning services would almost certainly be an effective strategy for reducing teenage pregnancies as well as unplanned pregnancies among older women.
Another strategy to prevent teenage pregnancy involves the use of early childhood intervention (ECI) programs. Many such programs exist, but they generally include visits by social workers, nurses, and other professionals to the homes of children who are at risk for neurological, emotional, and/or behavioral problems during their first several years and also as they grow into adolescents and young adults (Kahn & Moore, 2010). It might sound like a stereotype, but these children are disproportionately born to single, teenage mothers and/or to slightly older parents who live in poverty or near poverty. Long-term evaluation studies show that the best of these programs reduce the likelihood that the very young children they help will become pregnant or have children of their own after they become teenagers (Ball & Moore, 2008). In effect, assisting young children to today helps prevent teenage pregnancy tomorrow.
The second prong to this harm reduction strategy targets teenage parents and their children. Because teen pregnancies occur despite the best prevention efforts, the second goal of a harm reduction approach is to help teens during their pregnancy and after childbirth. This strategy has the immediate aim of providing practical and emotional support for these very young mothers; it also has the longer-term goals of reducing repeat pregnancies and births and of preventing developmental and behavior problems among their children.
To achieve these aims, Early Childhood Intervention programs have again been shown to be helpful (Ball & Moore, 2008). Another type of program to help teen mothers involves the use of second-chance homes, which are maternity group homes for unmarried teen mothers (Andrews & Moore, 2011). One of the many sad facts of teenage motherhood is that teen mothers often have nowhere to live. A teen mother’s parent(s) may refuse to let her and her infant live with them, either because they are angry at her pregnancy or because they simply do not have the room or financial means to house and take care of a baby. Or a pregnant teen may decide to leave her parents’ home because of the parents’ anger or because they refuse to let her continue seeing the child’s father. In another possibility, a teen mother may begin living with the father, but these unions are typically unstable and often end, again leaving her and her child without a home. As well, many teen mothers were runaways from home before they became pregnant or were living in foster care. Because of all these situations, many teen mothers find themselves without a place to live.
In second-chance homes (which, depending on the program, are in reality one large house, a set of apartments, or a network of houses), mothers and children (as well as pregnant teens) receive shelter and food, but they also receive essential services, such as childrearing help, educational and vocational counseling and training, family planning counseling, and parenting classes. Although rigorous evaluation studies do not yet exist on the effectiveness of second-chance homes, they do seem to offer a valuable resource for teen mothers and their children (Andrews & Moore, 2011).
A final strategy for addressing the problem of teenage sex and pregnancy is to address a more general societal condition that helps produce teenage sex and pregnancy. This condition is poverty. As noted earlier, children who grow up in poor families and in disadvantaged neighborhoods—those with high rates of poverty, unemployment, high school dropouts, and so forth—are more likely to have sex earlier as teens and to become pregnant (Harding, 2003).
Sexually Transmitted Infections
In addition to pregnancy and birth, another problem associated with teenage sexual activity is the transmission of sexually transmitted infections (STIs). This is a problem during the teenage years, but it is even more of a problem during young adulthood, when sexual activity is higher than during adolescence (Wildsmith, Schelar, Peterson, & Manlove, 2010). The STI rate in the United States is higher than in most other Western democracies. Almost 19 million new cases of STIs are diagnosed annually, and more than 65 million Americans have an incurable STI, such as herpes. Although teens and young adults ages 15–24 compose only one-fourth of sexually active people, they account for one-half of all new STIs. Despite this fact, most young adults who test positive for an STI did not believe they were at risk of getting an STI (Wildsmith et al., 2010).
In any one year, 15 percent of young adults ages 18 and 26 have an STI. This figure masks a significant gender difference: 20 percent of young women have had an STI in the past year, compared to 10 percent of young men. It also masks important racial/ethnic differences: 34 percent of young African Americans have had an STI in the past year, compared to 10 percent of Asians, 15 percent of Hispanics, and 10 percent of whites.
Three types of sexual behaviors increase the risk of transmitting or contracting an STI: having sex with at least three partners during the past year, having a sex partner with a known STI, and not using a condom regularly. About 17 percent of sexually active young adults have had at least three partners during the past year, and 8 percent have had a partner with a known STI. Three-fourths of unmarried sexually active young adults do not use a condom regularly. Combining all these risk factors, 39 percent have engaged in one risk factor in the past year, 14 percent have engaged in at least two risk factors, and the remainder, 48 percent, have engaged in no risk factors (Wildsmith et al., 2010).
Think About It
- Imagine that you became a parent at age 17. How would your life have been different from what it is now?
- Many sexually active teenagers do not use contraception regularly. Why do you think they do not use it more often?
Developing sexually is an expected and natural part of growing into adulthood. Healthy sexual development involves more than sexual behavior. It is the combination of physical sexual maturation (puberty, age-appropriate sexual behaviors), the formation of a positive sexual identity, and a sense of sexual well-being (discussed more in-depth later in this module). During adolescence, teens strive to become comfortable with their changing bodies and to make healthy, safe decisions about which sexual activities, if any, they wish to engage in.
Earlier in the physical development section, we discussed primary and secondary sex characteristics. During puberty, every primary sex organ (the ovaries, uterus, penis, and testes) increases dramatically in size and matures in function. During puberty, reproduction becomes possible. Simultaneously, secondary sex characteristics develop. These characteristics are not required for reproduction, but they do signify masculinity and femininity. At birth, boys and girls have similar body shapes, but during puberty, males widen at the shoulders, and females widen at the hips and develop breasts (examples of secondary sex characteristics). Sexual development is impacted by a dynamic mixture of physical and cognitive change, coupled with social expectations. With physical maturation, adolescents may become alternately fascinated with and chagrined by their changing bodies, and often compare themselves to the development they notice in their peers or see in the media. For example, many adolescent girls focus on their breast development, hoping their breasts will conform to an ideal body image.
As sex hormones cause biological changes, they also affect the brain and trigger sexual thoughts. Culture, however, shapes actual sexual behaviors. Emotions regarding sexual experience, like the rest of puberty, are strongly influenced by cultural norms regarding what is expected at what age, with peers being the most influential. Simply put, the most important influence on adolescents’ sexual activity is not their bodies, but their close friends, who have more influence than do sex or ethnic group norms (van de Bongardt et al., 2015).
Sexual interest and interaction are a natural part of adolescence. Sexual fantasy and masturbation episodes increase between the ages of 10 and 13. Masturbation is very ordinary—even young children have been known to engage in this behavior. As the bodies of children mature, powerful sexual feelings begin to develop, and masturbation helps release sexual tension. For adolescents, masturbation is a common way to explore their erotic potential, and this behavior can continue throughout adult life.
https://youtu.be/QZWd-fhmqmQ
Video 3.4.1. "What Happens When?" Child and Adolescent Sexual Development explains major milestones in sexual development throughout childhood and adolescence, as well as how to support kids during these stages.
Sexual Interactions
Many early social interactions tend to be nonsexual—text messaging, phone calls, email—but by the age of 12 or 13, some young people may pair off and begin dating and experimenting with kissing, touching, and other physical contact, such as oral sex. The vast majority of young adolescents are not prepared emotionally or physically for oral sex and sexual intercourse. If adolescents this young do have sex, they are highly vulnerable to sexual and emotional abuse, sexually transmitted infections (STIs), HIV, and early pregnancy. For STI’s in particular, adolescents are slower to recognize symptoms, tell partners, and get medical treatment, which puts them at risk of infertility and even death.
Adolescents ages 14 to 16 understand the consequences of unprotected sex and teen parenthood, if properly taught, but cognitively they may lack the skills to integrate this knowledge into everyday situations or consistently to act responsibly in the heat of the moment. By the age of 17, many adolescents have willingly experienced sexual intercourse. Teens who have early sexual intercourse report strong peer pressure as a reason behind their decision. Some adolescents are just curious about sex and want to experience it.
Becoming a sexually healthy adult is a developmental task of adolescence that requires integrating psychological, physical, cultural, spiritual, societal, and educational factors. It is particularly important to understand the adolescent in terms of his or her physical, emotional, and cognitive stage. Additionally, healthy adult relationships are more likely to develop when adolescent impulses are not shamed or feared. Guidance is certainly needed, but acknowledging that adolescent sexuality development is both normal and positive would allow for more open communication so adolescents can be more receptive to education concerning the risks (Tolman & McClelland, 2011).
Adolescents are receptive to their culture, to the models they see at home, in school, and in the mass media. These observations influence moral reasoning and moral behavior, which we discuss in more detail later in this module. Decisions regarding sexual behavior are influenced by teens’ ability to think and reason, their values, and their educational experience. Helping adolescents recognize all aspects of sexual development encourages them to make informed and healthy decisions about sexual matters.
Teenage Sexual Activity Trends
Teenagers are much more sexually active today than they were before the sexual revolution of the 1960s and 70s. About 43 percent of never-married teens ages 15–19 of both sexes have had sexual intercourse (Martinez et al., 2011); this percentage represents a drop from its highest point, in 1988, of 51 percent for females and of 60 percent for males. About three-fourths of girls in today’s sexually experienced group and 85 percent of boys in this group use contraception, most often a condom, the first time they ever have sex. In their most recent act of sexual intercourse, almost 86 percent of girls and 93 percent of boys used contraception, again most often a condom.
If 43 percent of teens have had sexual intercourse, that means the majority of teens, 57 percent, have never had intercourse. It is interesting to examine their reasons. The table below identifies the main reason given for never having sexual intercourse. The top reason for both sexes is religion and morals, followed by concern about a possible pregnancy and not having found the right person with whom to have sex (Martinez et al., 2011).
Table 3.4.1. Main Reason Given for Never Having Sexual Intercourse, Ages 15–19 (%)
| Females | Males | |
| Against religion or morals | 38 | 31 |
| Don’t want to get (a female) pregnant | 19 | 25 |
| Haven’t found the right person yet | 17 | 21 |
| Don’t want to get an STI | 7 | 10 |
| In a relationship, but waiting for the right time | 7 | 5 |
| Other reason | 12 | 8 |
The Problem of Teenage Pregnancy
Most teenage pregnancies and births are unplanned and are part of a more general problem for all women in their childbearing years. Almost 700,000 unplanned teenage pregnancies occur annually; another 50,000 teenage pregnancies are planned. These 750,000 teenage pregnancies annually result in some 400,000 births (Kost, Henshaw, & Carlin, 2010). Altogether, about 18 percent of women, or one of every six females, become teen mothers, and in several southern and southwestern states, this percentage is as high as 25–30 percent (Perper & Manlove, 2009).
The birth rate for females aged 15–19 in 2009 was 39.1 births per 1,000 females. This rate represented a substantial decline from the early 1990s when the rate reached a peak of almost 60. However, it was still twice as high as Canada’s rate and much higher yet than other Western democracies (Figure 3.4.1).
Figure 3.4.1. Teenage Birth Rates in Selected Western Democracies
Although teenaged pregnancies (and births from these pregnancies) are far from the majority of all pregnancies, unplanned or planned, they pose special problems (American College of Obstetricians and Gynecologists, 2011; Anderson, 2014). On the individual level, pregnant teenagers are more at risk than older pregnant women for high blood pressure and anemia, and they are also more likely to experience early labor, premature birth, and low birth weight. In addition, because teenagers are more likely than adults to have STIs, pregnant teenagers are more likely than older pregnant women to have an STI while they are pregnant, either because they already had an STI when they conceived or because they contract an STI from having sex during pregnancy.
Many pregnant teenagers decide to drop out of school. If they stay in school, they often must deal with the embarrassment of being pregnant, and the physical and emotional difficulties accompanying their teenage pregnancy can affect their school performance. Once the baby is born, child care typically becomes an enormous problem, whether or not the new mother is in school. Because pregnant teenagers disproportionately come from families that are poor or near-poor, they have few financial resources and often have weak social support networks, either before or after the baby is born (Andrews & Moore, 2011).
At the societal level, teenage pregnancy and motherhood are very costly in at least two important respects. First, because pregnancy and childbirth complications are more common among teenagers, their health-care expenses during and after pregnancy and childbirth are often higher than the expenses incurred by older women. Medicaid, the federal government’s national health plan for poor families, often covers much of these expenses, and the premiums that private health insurance companies charge are higher than otherwise because of their expenses when they insure the families of pregnant teenagers.
Second, the children of teenage mothers are at risk for several kinds of behavioral and developmental problems. Teenage parents may be unprepared emotionally or practically to raise a child. Children of teen parents may receive less cognitive stimulation and proper emotional support. In addition, the stress they experience as young parents put them at risk of neglecting or abusing their children. Teenage parents also tend to come from low-income families and continue to live in poverty or near poverty after they become mothers compounds all these problems. For all these reasons, the children of teenage mothers are at greater risk for several kinds of issues. These problems include impaired neurological development, behavioral problems, poor school performance, and chronic health problems.
Reducing Teenage Pregnancy
In an effort to reduce teenage pregnancies, two approaches have been used: (1) Emphasize abstinence, convincing teens to hold off on having sex until adulthood or marriage, and (2) comprehensive sex education, including teaching the effective use of contraception if they do have sex. Most sexual behavior researchers believe that pleas for abstinence, as well as sex education programs that focus solely or almost entirely on abstinence, do not help to reduce teen sex and pregnancy (Ball & Moore, 2008).
Comprehensive sex education is based on the strategy of harm reduction. A harm reduction approach recognizes that because certain types of harmful behavior are inevitable, our society should do its best to minimize the various kinds of harm that these various behaviors generate. In regard to teenage sex and pregnancy, a harm reduction approach has two goals: (1) to help reduce the risk for pregnancy among sexually active teens and (2) to help teenage parents and their children.
To achieve the first goal, parents, sex education classes, family planning clinics, youth development programs, and other parties must continue to emphasize the importance of waiting to have sex but also the need for teenagers to use contraception if they are sexually active. In addition, effective contraception (birth control pills, other hormonal control, and even condoms, which protect against STIs) must be made available for teenagers at little or no cost. Studies indicate that these two contraception strategies do not lead to more teenage sex, and they also indicate that consistent contraceptive use dramatically reduces the risk of teenage pregnancy. As one writer has summarized these studies’ conclusions, “Contraceptives no more cause sex than umbrellas cause rain…When contraception is unavailable, the likely consequences is not less sex, but more pregnancy” (Kristof, 2011, p. A31).
In this regard, a recent report of the Guttmacher Institute called contraception a “proven, cost-effective strategy” (Gold, 2011, p. 7). It added, “Contraception is almost universally accepted as a way to reduce the risk of unintended pregnancy…Contraceptive use reduces the risk of unintended pregnancy significantly, and consistent contraceptive use virtually eliminates it.” The report noted that government-funded family planning agencies prevent 2 million unintended pregnancies annually by providing contraception to 9 million young and low-income women each year. Because most of the women who would have these prevented pregnancies would be eligible for Medicaid, the Medicaid savings from these prevented pregnancies amount to about $7 billion annually. An expansion of family planning services would almost certainly be an effective strategy for reducing teenage pregnancies as well as unplanned pregnancies among older women.
Another strategy to prevent teenage pregnancy involves the use of early childhood intervention (ECI) programs. Many such programs exist, but they generally include visits by social workers, nurses, and other professionals to the homes of children who are at risk for neurological, emotional, and/or behavioral problems during their first several years and also as they grow into adolescents and young adults (Kahn & Moore, 2010). It might sound like a stereotype, but these children are disproportionately born to single, teenage mothers and/or to slightly older parents who live in poverty or near poverty. Long-term evaluation studies show that the best of these programs reduce the likelihood that the very young children they help will become pregnant or have children of their own after they become teenagers (Ball & Moore, 2008). In effect, assisting young children to today helps prevent teenage pregnancy tomorrow.
The second prong to this harm reduction strategy targets teenage parents and their children. Because teen pregnancies occur despite the best prevention efforts, the second goal of a harm reduction approach is to help teens during their pregnancy and after childbirth. This strategy has the immediate aim of providing practical and emotional support for these very young mothers; it also has the longer-term goals of reducing repeat pregnancies and births and of preventing developmental and behavior problems among their children.
To achieve these aims, Early Childhood Intervention programs have again been shown to be helpful (Ball & Moore, 2008). Another type of program to help teen mothers involves the use of second-chance homes, which are maternity group homes for unmarried teen mothers (Andrews & Moore, 2011). One of the many sad facts of teenage motherhood is that teen mothers often have nowhere to live. A teen mother’s parent(s) may refuse to let her and her infant live with them, either because they are angry at her pregnancy or because they simply do not have the room or financial means to house and take care of a baby. Or a pregnant teen may decide to leave her parents’ home because of the parents’ anger or because they refuse to let her continue seeing the child’s father. In another possibility, a teen mother may begin living with the father, but these unions are typically unstable and often end, again leaving her and her child without a home. As well, many teen mothers were runaways from home before they became pregnant or were living in foster care. Because of all these situations, many teen mothers find themselves without a place to live.
In second-chance homes (which, depending on the program, are in reality one large house, a set of apartments, or a network of houses), mothers and children (as well as pregnant teens) receive shelter and food, but they also receive essential services, such as childrearing help, educational and vocational counseling and training, family planning counseling, and parenting classes. Although rigorous evaluation studies do not yet exist on the effectiveness of second-chance homes, they do seem to offer a valuable resource for teen mothers and their children (Andrews & Moore, 2011).
A final strategy for addressing the problem of teenage sex and pregnancy is to address a more general societal condition that helps produce teenage sex and pregnancy. This condition is poverty. As noted earlier, children who grow up in poor families and in disadvantaged neighborhoods—those with high rates of poverty, unemployment, high school dropouts, and so forth—are more likely to have sex earlier as teens and to become pregnant (Harding, 2003).
Sexually Transmitted Infections
In addition to pregnancy and birth, another problem associated with teenage sexual activity is the transmission of sexually transmitted infections (STIs). This is a problem during the teenage years, but it is even more of a problem during young adulthood, when sexual activity is higher than during adolescence (Wildsmith, Schelar, Peterson, & Manlove, 2010). The STI rate in the United States is higher than in most other Western democracies. Almost 19 million new cases of STIs are diagnosed annually, and more than 65 million Americans have an incurable STI, such as herpes. Although teens and young adults ages 15–24 compose only one-fourth of sexually active people, they account for one-half of all new STIs. Despite this fact, most young adults who test positive for an STI did not believe they were at risk of getting an STI (Wildsmith et al., 2010).
In any one year, 15 percent of young adults ages 18 and 26 have an STI. This figure masks a significant gender difference: 20 percent of young women have had an STI in the past year, compared to 10 percent of young men. It also masks important racial/ethnic differences: 34 percent of young African Americans have had an STI in the past year, compared to 10 percent of Asians, 15 percent of Hispanics, and 10 percent of whites.
Three types of sexual behaviors increase the risk of transmitting or contracting an STI: having sex with at least three partners during the past year, having a sex partner with a known STI, and not using a condom regularly. About 17 percent of sexually active young adults have had at least three partners during the past year, and 8 percent have had a partner with a known STI. Three-fourths of unmarried sexually active young adults do not use a condom regularly. Combining all these risk factors, 39 percent have engaged in one risk factor in the past year, 14 percent have engaged in at least two risk factors, and the remainder, 48 percent, have engaged in no risk factors (Wildsmith et al., 2010).
Think About It
- Imagine that you became a parent at age 17. How would your life have been different from what it is now?
- Many sexually active teenagers do not use contraception regularly. Why do you think they do not use it more often?
Aiken, L. R. (1996). Assessment of intellectual functioning. Springer Science & Business Media.
Albert, D., & Steinberg, L. (2011). Judgment and decision making in adolescence. Journal of research on Adolescence, 21(1), 211-224.
Alloway, T. P. (2009). Working memory, but not IQ, predicts subsequent learning in children with learning difficulties. European journal of psychological assessment, 25(2), 92-98.
Alloway, T. P., Bibile, V., & Lau, G. (2013). Computerized working memory training: Can it lead to gains in cognitive skills in students?. Computers in Human Behavior, 29(3), 632-638.
Anderson, S. R. (1969). West Scandinavian vowel systems and the ordering of phonological rules (Doctoral dissertation, Massachusetts Institute of Technology).
Atkinson, R. C., & Shiffrin, R. M. (1968). Human memory: A proposed system and its control processes. In Psychology of learning and motivation (Vol. 2, pp. 89-195). Academic press.
Bibok, M. B., Carpendale, J. I., & Müller, U. (2009). Parental scaffolding and the development of executive function. New directions for child and adolescent development, 2009(123), 17-34.
Bink, M. L., & Marsh, R. L. (2000). Cognitive regularities in creative activity. Review of General Psychology, 4(1), 59-78.
Bjorklund, A., Jantti, M., & Solon, G. (2005). Influences of nature and nurture on earnings variation. Unequal chances: Family background and economic success, 145, 164.
Brody, S. D. (2003). Are we learning to make better plans? A longitudinal analysis of plan quality associated with natural hazards. Journal of Planning Education and Research, 23(2), 191-201.
Case, R., Okamoto, Y., Griffin, S., McKeough, A., Bleiker, C., Henderson, B., ... & Keating, D. P. (1996). The role of central conceptual structures in the development of children's thought. Monographs of the society for research in child development, i-295.
Carlson, S. M., Zelazo, P. D., & Faja, S. (2013). Executive function.
Collet, C., Clarion, A., Morel, M., Chapon, A., & Petit, C. (2009). Physiological and behavioural changes associated to the management of secondary tasks while driving. Applied ergonomics, 40(6), 1041-1046.
Crain, W. (2007). Homework and the Freedom to Think. Reading Against Democracy: The Broken Promises of Reading Instruction, 20(4), 30.
de Ribaupierre, A. (2001). Working memory and attentional processes across the lifespan. Lifespan development of human memory, 59-80.
Elkind, D. (1967). Egocentrism in adolescence. Child development, 1025-1034.
Ennis, R. H. (1987). Critical thinking and the curriculum. Thinking skills instruction: Concepts and techniques, 40-48.
Ericsson, K. A. (1998). The scientific study of expert levels of performance: General implications for optimal learning and creativity. High Ability Studies, 9(1), 75-100.
Fay‐Stammbach, T., Hawes, D. J., & Meredith, P. (2014). Parenting influences on executive function in early childhood: A review. Child development perspectives, 8(4), 258-264.
Kail, R. V., McBride‐Chang, C., Ferrer, E., Cho, J. R., & Shu, H. (2013). Cultural differences in the development of processing speed. Developmental science, 16(3), 476-483.
Gardner, H. (1983). Artistic intelligences. Art Education, 36(2), 47-49.
Garlick, D. (2002). Understanding the nature of the general factor of intelligence: the role of individual differences in neural plasticity as an explanatory mechanism. Psychological review, 109(1), 116.
Greenspan, S., Loughlin, G., & Black, R. S. (2001). Credulity and gullibility in people with developmental disorders: A framework for future research. In International review of research in mental retardation (Vol. 24, pp. 101-135). Academic Press.
Gottfredson, L. S. (1997). Why g matters: The complexity of everyday life. Intelligence, 24(1), 79-132.
Guy, J., Rogers, M., & Cornish, K. (2013). Age-related changes in visual and auditory sustained attention in preschool-aged children. Child Neuropsychology, 19(6), 601-614.
Hassabis, D., & Maguire, E. A. (2007). Deconstructing episodic memory with construction. Trends in cognitive sciences, 11(7), 299-306.
Hennessey, B. A., & Amabile, T. M. (2016). Intrinsic Motivation and Creativity in the Classroom. Nurturing creativity in the classroom.
Herrmann, E., Misch, A., Hernandez‐Lloreda, V., & Tomasello, M. (2015). Uniquely human self‐control begins at school age. Developmental science, 18(6), 979-993.
Herrmann, E., & Tomasello, M. (2015). Focusing and shifting attention in human children (Homo sapiens) and chimpanzees (Pan troglodytes). Journal of Comparative Psychology, 129(3), 268.
Hitch, G. J., & Baddeley, A. D. (1976). Verbal reasoning and working memory. The Quarterly Journal of Experimental Psychology, 28(4), 603-621.
Jones, P. R., Moore, D. R., & Amitay, S. (2015). Development of auditory selective attention: why children struggle to hear in noisy environments. Developmental psychology, 51(3), 353.
Kahneman, D. (2011). Fast and slow thinking. Allen Lane and Penguin Books, New York.
Klaczynski, P. A. (2001). Analytic and heuristic processing influences on adolescent reasoning and decision‐making. Child development, 72(3), 844-861.
Klaczynski, P. A., & Felmban, W. S. (2014). Adolescent development: Heuristics, biases, and individual differences. The developmental psychology of reasoning and decision‐making, 84-112.
Kuhn, D., Zillmer, N., Crowell, A., & Zavala, J. (2013). Developing norms of argumentation: Metacognitive, epistemological, and social dimensions of developing argumentive competence. Cognition and Instruction, 31(4), 456-496.
Lally, M. J., & Valentine-French, S. J. (2015). Introduction to Psychology [Adapted from Charles Stangor, Introduction to Psychology] Grayslake. IL: College of Lake County.
|
Lubinski, D., & Benbow, C. P. (2006). Study of mathematically precocious youth after 35 years: Uncovering antecedents for the development of math-science expertise. Perspectives on psychological science, 1(4), 316-345.
|
Matlin, M. W. (2013). Margaret W. Matlin. In Models of Achievement (pp. 239-254). Psychology Press.
Nelson, K., & Fivush, R. (2004). The emergence of autobiographical memory: a social cultural developmental theory. Psychological review, 111(2), 486.
Oden, M. H. (1968). The fulfillment of promise: 40 year follow up of the Terman gifted group. Stanford University Press.
Peng, P., Namkung, J., Barnes, M., & Sun, C. (2016). A meta-analysis of mathematics and working memory: Moderating effects of working memory domain, type of mathematics skill, and sample characteristics. Journal of Educational Psychology, 108(4), 455.
Piaget, J., & Inhelder, B. (2014). Intellectual operations and their development. In Experimental Psychology Its Scope and Method: Volume VII (Psychology Revivals) (pp. 144-205). Psychology Press.
Porporino, M., Iarocci, G., Shore, D. I., & Burack, J. A. (2004). A developmental change in selective attention and global form perception. International Journal of Behavioral Development, 28(4), 358-364.
Posner, M. I., & Rothbart, M. K. (2007). Research on attention networks as a model for the integration of psychological science. Annu. Rev. Psychol., 58(1), 1-23.
Raichle, M. E. (2015). The brain's default mode network. Annual review of neuroscience, 38(1), 433-447.
Rueda, M. R., Rothbart, M. K., McCandliss, B. D., Saccomanno, L., & Posner, M. I. (2005). Training, maturation, and genetic influences on the development of executive attention. Proceedings of the National Academy of Sciences, 102(41), 14931-14936.
Salvucci, D. D., & Taatgen, N. A. (2008). Threaded cognition: an integrated theory of concurrent multitasking. Psychological review, 115(1), 101.
Seagoe, M. V. (1975). Terman and the gifted. William Kaufman.
Schneider, W., Kron-Sperl, V., & Hünnerkopf, M. (2009). The development of young children's memory strategies: Evidence from the Würzburg Longitudinal Memory Study. European Journal of Developmental Psychology, 6(1), 70-99.
Schwartz, P. D., Maynard, A. M., & Uzelac, S. M. (2008). Adolescent egocentrism: a contemporary view. Adolescence, 43(171), 441-449.
Siegler, R. S. (1992). The Other Alfred Binet. Developmental psychology, 28(2), 179.
Siegler, R. S. (1998). Emerging minds: The process of change in children's thinking. Oxford University Press.
Simonton, D. K. (2000). Creativity: Cognitive, personal, developmental, and social aspects. American psychologist, 55(1), 151.
Sinnott, J. (1998). The development of logic in adulthood: Postformal thought and its applications. Springer Science & Business Media.
Sodian, B., & Schneider, W. (1999). Memory strategy development: Gradual increase, sudden insight, or roller coaster. Individual development from, 3, 61-77.
Sternberg, R. J. (2003). Wisdom, intelligence, and creativity synthesized. Cambridge University Press.
Sternberg, R. J. (2012). The assessment of creativity: An investment-based approach. Creativity research journal, 24(1), 3-12.
Strayer, D. L., & Drews, F. A. (2007). Cell-phone–induced driver distraction. Current Directions in Psychological Science, 16(3), 128-131.
Tarasova, I. V., Volf, N. V., & Razoumnikova, O. M. (2010). Parameters of cortical interactions in subjects with high and low levels of verbal creativity. Human Physiology, 36, 80-85.
Treffert, D. A., & Wallace, G. L. (2004). Islands of genius. Scientific American Mind, 14(1), 14-23.
Tulving, E. (1972). Episodic and semantic memory. Organization of memory, 1(381-403), 1.
Tulving, E. (2002). Episodic memory: From mind to brain. Annual review of psychology, 53(1), 1-25.
Vakil, E., Greenstein, Y., & Blachstein, H. (2010). Normative data for composite scores for children and adults derived from the Rey Auditory Verbal Learning Test. The Clinical Neuropsychologist, 24(4), 662-677.
Vygotsky, L. S. (1962). Language and thought (pp. 11193-000). Cambridge, MA: MIT Press.
Wagner, R. K., & Sternberg, R. J. (1985). Practical intelligence in real-world pursuits: The role of tacit knowledge. Journal of personality and social psychology, 49(2), 436.
Weisberg, M. K., McCoy, T. J., & Krot, A. N. (2006). Systematics and evaluation of meteorite classification. Meteorites and the early solar system II, 19, 19-52.
 Lev Vygotsky (1896-1934) was a Russian psychologist whose sociocultural theory emphasizes the importance of culture and interaction in the development of cognitive abilities. Vygotsky differed with Piaget in that he believed that a person has not only a set of abilities but also a set of potential abilities that can be realized if given the proper guidance from others. Vygotsky developed theories on teaching that have been adopted by educators today.
Lev Vygotsky (1896-1934) was a Russian psychologist whose sociocultural theory emphasizes the importance of culture and interaction in the development of cognitive abilities. Vygotsky differed with Piaget in that he believed that a person has not only a set of abilities but also a set of potential abilities that can be realized if given the proper guidance from others. Vygotsky developed theories on teaching that have been adopted by educators today.
Like Piaget, Vygotsky acknowledged intrinsic development, but he argued that it is the language, writings, and concepts arising from the culture that elicit the highest level of cognitive thinking (Crain, 2007). He believed that social interactions with teachers and more learned peers could facilitate a learner's potential for learning. Without this interpersonal instruction, he believed learner's minds would not advance very far as their knowledge would be based only on their own discoveries.
Figure 5.2.1. Lev Vygotsky
Zone of Proximal Development and Scaffolding
Vygotsky's best-known concept is the Zone of Proximal Development (ZPD). The ZPD has been defined as "the distance between the actual developmental level as determined by independent problem solving and the level of potential development as determined through problem-solving under adult guidance, or in collaboration with more capable peers" (Vygotsky, 1978, p. 86). Vygotsky stated that learners should be taught in the ZPD. A good teacher or more-knowledgable-other (MKO) identifies a learner's ZPD and helps them stretch beyond it. Then the MKO gradually withdraws support until the learner can perform the task unaided. Other psychologists have applied the metaphor of scaffolds (the temporary platforms on which construction workers stand) to Vygotsky's theory. Scaffolding is the temporary support that a MKO gives a learner to do a task.

Figure 5.2.2. Model of Vygotsky's zone of proximal development.
Thought and Speech
Do you ever talk to yourself? Why? Chances are, this occurs when you are struggling with a problem, trying to remember something, or feel very emotional about a situation. Children talk to themselves too. Piaget interpreted this as egocentric speech or a practice engaged in because of a child's inability to see things from another's point of view. Vygotsky, however, believed that children talk to themselves in order to solve problems or clarify thoughts. As children learn to think in words, they do so aloud, referred to as private speech, speech meant only for one's self. Eventually, thinking out loud becomes thought accompanied by internal speech, and talking to oneself becomes a practice only engaged in when we are trying to learn something or remember something. This inner speech is not as elaborate as the speech we use when communicating with others (Vygotsky, 1962).
Vygotsky's Influence on Education
Vygotsky’s theories have been extremely influential for education. Although Vygotsky himself never mentioned the term scaffolding, it is often credited to him as a continuation of his ideas pertaining to the way adults or other children can use guidance in order for a child to work within their ZPD. (The term scaffolding was first developed by Jerome Bruner, David Wood, and Gail Ross while applying Vygotsky’s concept of ZPD to various educational contexts.)
Educators often apply these concepts by assigning tasks that students cannot do on their own, but which they can do with assistance; they should provide just enough assistance so that students learn to complete the tasks independently and then provide an environment that enables students to do harder tasks than would otherwise be possible. Teachers can also allow students with more knowledge to assist students who need more guidance. Especially in the context of collaborative learning, group members who have higher levels of understanding can help the less advanced members learn within their zone of proximal development.
https://youtu.be/InzmZtHuZPY
Video 5.2.1. Vygotsky's Developmental Theory introduces the applications of the theory in the classroom.
Case, R., Okamoto, Y., Griffin, S., McKeough, A., Bleiker, C., Henderson, B., ... & Keating, D. P. (1996). The role of central conceptual structures in the development of children's thought. Monographs of the society for research in child development, i-295.
Carlson, S. M., Zelazo, P. D., & Faja, S. (2013). Executive function.
Collet, C., Clarion, A., Morel, M., Chapon, A., & Petit, C. (2009). Physiological and behavioural changes associated to the management of secondary tasks while driving. Applied ergonomics, 40(6), 1041-1046.
Crain, W. (2007). Homework and the Freedom to Think. Reading Against Democracy: The Broken Promises of Reading Instruction, 20(4), 30.
Elkind, D. (1967). Egocentrism in adolescence. Child development, 1025-1034.
Guy, J., Rogers, M., & Cornish, K. (2013). Age-related changes in visual and auditory sustained attention in preschool-aged children. Child Neuropsychology, 19(6), 601-614.
Herrmann, E., Misch, A., Hernandez‐Lloreda, V., & Tomasello, M. (2015). Uniquely human self‐control begins at school age. Developmental science, 18(6), 979-993.
Herrmann, E., & Tomasello, M. (2015). Focusing and shifting attention in human children (Homo sapiens) and chimpanzees (Pan troglodytes). Journal of Comparative Psychology, 129(3), 268.
Jones, P. R., Moore, D. R., & Amitay, S. (2015). Development of auditory selective attention: why children struggle to hear in noisy environments. Developmental psychology, 51(3), 353.
Klaczynski, P. A., & Felmban, W. S. (2014). Adolescent development: Heuristics, biases, and individual differences. The developmental psychology of reasoning and decision‐making, 84-112.
Kuhn, D., Zillmer, N., Crowell, A., & Zavala, J. (2013). Developing norms of argumentation: Metacognitive, epistemological, and social dimensions of developing argumentive competence. Cognition and Instruction, 31(4), 456-496.
Matlin, M. W. (2013). Margaret W. Matlin. In Models of Achievement (pp. 239-254). Psychology Press.
Nelson, K., & Fivush, R. (2004). The emergence of autobiographical memory: a social cultural developmental theory. Psychological review, 111(2), 486.
Piaget, J., & Inhelder, B. (2014). Intellectual operations and their development. In Experimental Psychology Its Scope and Method: Volume VII (Psychology Revivals) (pp. 144-205). Psychology Press.
Porporino, M., Iarocci, G., Shore, D. I., & Burack, J. A. (2004). A developmental change in selective attention and global form perception. International Journal of Behavioral Development, 28(4), 358-364.
Posner, M. I., & Rothbart, M. K. (2007). Research on attention networks as a model for the integration of psychological science. Annu. Rev. Psychol., 58(1), 1-23.
Raichle, M. E. (2015). The brain's default mode network. Annual review of neuroscience, 38(1), 433-447.
Rueda, M. R., Rothbart, M. K., McCandliss, B. D., Saccomanno, L., & Posner, M. I. (2005). Training, maturation, and genetic influences on the development of executive attention. Proceedings of the National Academy of Sciences, 102(41), 14931-14936.
Salvucci, D. D., & Taatgen, N. A. (2008). Threaded cognition: an integrated theory of concurrent multitasking. Psychological review, 115(1), 101.
Schwartz, P. D., Maynard, A. M., & Uzelac, S. M. (2008). Adolescent egocentrism: a contemporary view. Adolescence, 43(171), 441-449.
Sinnott, J. (1998). The development of logic in adulthood: Postformal thought and its applications. Springer Science & Business Media.
Sternberg, R. J. (2012). The assessment of creativity: An investment-based approach. Creativity research journal, 24(1), 3-12.
Strayer, D. L., & Drews, F. A. (2007). Cell-phone–induced driver distraction. Current Directions in Psychological Science, 16(3), 128-131.
Vakil, E., Greenstein, Y., & Blachstein, H. (2010). Normative data for composite scores for children and adults derived from the Rey Auditory Verbal Learning Test. The Clinical Neuropsychologist, 24(4), 662-677.
Vygotsky, L. S. (1962). Language and thought (pp. 11193-000). Cambridge, MA: MIT Press.
Information Processing is how individuals perceive, analyze, manipulate, use, and remember information. Unlike Piaget's theory, this approach proposes that cognitive development is ongoing and gradual, not organized into distinct stages. Some of the areas where we see changes include:
- Attention. Improvements are seen in selective attention(the process by which one focuses on one stimulus while tuning out another), as well as divided attention (the ability to pay attention to two or more stimuli at the same time).
- Memory. Improvements are seen in working memory and long-term memory.
- Processing Speed. With maturation, children think more quickly. Processing speed improves sharply between age five and middle adolescence, levels off around age 15, and does not appear to change between late adolescence and adulthood.
- Organization of Thinking. As children mature, they are more planful, they approach problems with strategy, and are flexible in using different strategies in different situations.
- Metacognition. Older children can think about thinking itself. This often involves monitoring one's own cognitive activity during the thinking process. Metacognitionprovides the ability to plan ahead, see the future consequences of an action, and provide alternative explanations of events.
Attention
Changes in attention have been described by many as the key to changes in human memory (Nelson & Fivush, 2004; Posner & Rothbart, 2007). However, attention is not a unified function; it is comprised of sub-processes. Our ability to focus on a single task or stimulus while ignoring distracting information, called selective attention. There is a sharp improvement in selective attention from age six into adolescence (Vakil, Blachstein, Sheinman, & Greenstein, 2009). Sustained attention is the ability to stay on task for long periods. The ability to switch our focus between tasks or external stimuli is called divided attention or multitasking, which also improves into adolescence (Carlson, Zelazo, & Faja, 2013).
https://youtu.be/s4JBqLoY3tY
Video 5.3.1. Attention explains the ways in which we may attend or fail to attend to stimuli.
Selective Attention
The ability with selective attention tasks improves through childhood and into adolescence. While children's selective attention may be inconsistent during middle childhood, adolescents demonstrate the ability to select and prioritize stimuli for attention reliably. The development of this ability is influenced by the child's temperament (Rothbart & Rueda, 2005), the complexity of the stimulus or task (Porporino, Shore, Iarocci & Burack, 2004), and may be dependent on whether the stimuli are visual or auditory (Guy, Rogers & Cornish, 2013). Guy et al. (2013) found that children's ability to attend to visual information selectively outpaced that of auditory stimuli. This change may explain why young children are not able to hear the voice of the teacher over the cacophony of sounds in the typical preschool classroom (Jones, Moore & Amitay, 2015). Jones and his colleagues found that 4 to 7 year-olds could not filter out background noise, especially when its frequencies were close in sound to the target sound. In comparison, teens often performed similarly to adults.
https://youtu.be/qpsaHE_uZic
Video 5.3.2. Theories of Selective Attention explains how and why we attend to some stimuli and not others.
Sustained Attention
Most measures of sustained attention typically ask individuals to spend several minutes focusing on one task, while waiting for an infrequent event, while there are multiple distractors for several minutes. Young children can retain their visual and auditory attention for approximately 5 minutes if they are 5-years-old, 6 minutes if they are 6-years old, 7 minutes if they are 7-years-old, and so on. If a task is interesting or novel, the child may sustain attention substantially longer. Sustained attention improves to around age 10, then plateaus with only small improvements to adulthood. Common estimates of the attention span of healthy teenagers and adults range from 10 to 20 minutes. There is some debate as to whether attention is consistently sustained or whether people repeatedly choose to re-focus on the same thing (Raichle, 2015) This ability to renew attention permits people to 'pay attention' to things that last for more than a few minutes.
For time-on-task measurements, the type of activity used in the test affects the results, as people are generally capable of a longer attention span when they are doing something that they find enjoyable or intrinsically motivating (Raichle,2015). Attention is also increased if the person can perform the task fluently, compared to a person who has difficulty performing the task, or to the same person when he or she is just learning the task. Fatigue, hunger, noise, and emotional stress reduce the time focused on the task. After losing attention from a topic, a person may restore it by resting, doing a different kind of activity, changing mental focus, or deliberately choosing to re-focus on the first topic.
Divided Attention
Divided attention can be thought of in a couple of ways. We may look at how well people can multitask, performing two or more tasks simultaneously, or how people can alternate attention between two or more tasks. For example, walking and talking to a friend at the same time is multitasking, where trying to text while driving requires us to alternate attention between two tasks quickly.
Young children (age 3-4) have considerable difficulties in dividing their attention between two tasks and often perform at levels equivalent to our closest relative, the chimpanzee. However, by age five, they have surpassed the chimp (Hermann, Misch, Hernandez-Lloreda & Tomasello, 2015; Hermann & Tomasello, 2015). Despite these improvements, 5-year-olds continue to perform below the level of school-age children, adolescents, and adults. These skills continue to develop into adolescence.
Regardless of age, we have a limited capacity for attention, and the division of attention is confined to that limitation. Our ability to effectively multitask or alternate attention is dependent on the automaticity or complexity of the task, but are also influenced by conditions like anxiety, arousal, task difficulty, and skills (Sternberg & Sternberg, 2012). Research shows that when dividing attention, people are more apt to make mistakes or perform their tasks more slowly (Matlin, 2013). Attention must be divided among all of the component tasks to perform them.
Classical research on divided attention involved people performing simultaneous tasks, like reading stories while listening and writing something else, or listening to two separate messages through different ears. Subjects were often tested on their ability to learn new information while engaged in multiple tasks. More current research examines the performance of doing two tasks simultaneously (Matlin, 2013), such as driving while performing another task. This research reveals that the human attentional system has limits for what it can process. For examples, driving performance is worse while engaged in other tasks; drivers make more mistakes, brake harder and later, get into more accidents, veer into other lanes, and/or are less aware of their surroundings when engaged in the previously discussed tasks (Collet et al., 2009; Salvucci & Taatgen, 2008; Strayer & Drews, 2007).
https://youtu.be/THJgaznSBu8
Video 5.3.3. The Spotlight Model of Attention and Our Ability to Multitask explains how we divide our attention to attend to different tasks or information.
Memory is an information processing system; therefore, we often compare it to a computer. Memory is the set of processes used to encode, store, and retrieve information over different periods of time.

Figure 5.5.1. Encoding involves the input of information into the memory system. Storage is the retention of encoded information. Retrieval, or getting the information out of memory and back into awareness, is the third function.
Encoding
We get information into our brains through a process called encoding, which is the input of information into the memory system. Once we receive sensory information from the environment, our brains label or code it. We organize the information with other similar information and connect new concepts to existing concepts. Encoding information occurs through automatic processing and effortful processing.
If someone asks you what you ate for lunch today, more than likely, you could recall this information quite easily. This is known as automatic processing, or the encoding of details like time, space, frequency, and the meaning of words. Automatic processing is usually done without any conscious awareness. Recalling the last time you studied for a test is another example of automatic processing. However, what about the actual test material that you studied? It probably required a lot of work and attention on your part in order to encode that information. This is known as effortful processing.
There are three types of encoding. The encoding of words and their meaning is known as semantic encoding. It was first demonstrated by William Bousfield (1935) in an experiment in which he asked people to memorize words. The 60 words were divided into 4 categories of meaning, although the participants did not know this because the words were randomly presented. When they were asked to remember the words, they tended to recall them in categories, showing that they paid attention to the meanings of the words as they learned them.
Visual encoding is the encoding of images, and acoustic encoding is the encoding of sounds, words in particular. To see how visual encoding works, read over this list of words: car, level, dog, truth, book, value. If you were asked later to recall the words from this list, which ones do you think you'd most likely remember? You would probably have an easier time recalling the words car, dog, and book, and a more difficult time recalling the words level, truth, and value. Why is this? Because you can recall images (mental pictures) more easily than words alone. When you read the words car, dog, and book, you created images of these things in your mind. These are concrete, high-imagery words. On the other hand, abstract words like level, truth, and value are low-imagery words. High-imagery words are encoded both visually and semantically (Paivio, 1986), thus building a more reliable memory.
Now let us turn our attention to acoustic encoding. You are driving in your car, and a song comes on the radio that you have not heard in at least ten years, but you sing along, recalling every word. In the United States, children often learn the alphabet through song, and they learn the number of days in each month through rhyme: "Thirty days hath September, / April, June, and November; / All the rest have thirty-one, / Save February, with twenty-eight days clear, / And twenty-nine each leap year." These lessons are easy to remember because of acoustic encoding. We encode the sounds the words make. This is one of the reasons why much of what we teach young children is done through song, rhyme, and rhythm.
Which of the three types of encoding do you think would give you the best memory of verbal information? Some years ago, psychologists Fergus Craik and Endel Tulving (1975) conducted a series of experiments to find out. Participants were given words along with questions about them. The questions required the participants to process the words at one of the three levels. The visual processing questions included such things as asking the participants about the font of the letters. The acoustic processing questions asked the participants about the sound or rhyming of the words, and the semantic processing questions asked the participants about the meaning of the words. After participants were presented with the words and questions, they were given an unexpected recall or recognition task.
Words that had been encoded semantically were better remembered than those encoded visually or acoustically. Semantic encoding involves a deeper level of processing than shallower visual or acoustic encoding. Craik and Tulving concluded that we process verbal information best through semantic encoding, especially if we apply what is called the self-reference effect. The self-reference effect is the tendency for an individual to have a better memory for information that relates to oneself in comparison to material that has less personal relevance (Rogers, Kuiper & Kirker, 1977). Could semantic encoding be beneficial to you as you attempt to memorize the concepts in this chapter?
https://youtu.be/mlrOJgyPySw
Video 5.5.1. Encoding Strategies discusses various encoding techniques that help us store information in memory.
Storage
Once the information has been encoded, we have to retain it somehow. Our brains take the encoded information and place it in storage. Storage is the creation of a permanent record of information.
In order for a memory to go into storage (i.e., long-term memory), it has to pass through three distinct stages: Sensory Memory, Short-Term Memory, and finally, Long-Term Memory. These stages were first proposed by Richard Atkinson and Richard Shiffrin (1968). Their model of human memory, called Atkinson-Shiffrin (A-S) or three-box model, is based on the belief that we process memories in the same way that a computer processes information.
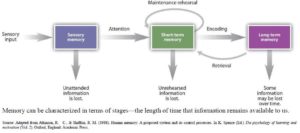
Figure 5.5.2. According to the Atkinson-Shiffrin model of memory, information passes through three distinct stages in order for it to be stored in long-term memory.
The three-box is just one model of memory. Others, such as Hitch and Baddeley (1976), have proposed a model where short-term memory itself has different forms. In this model, storing memories in short-term memory is like opening different files on a computer and adding information. The type of short-term memory (or computer file) depends on the type of information received. There are memories in visual-spatial form, as well as memories of spoken or written material, and they are stored in three short-term systems: a visuospatial sketchpad, an episodic buffer, and a phonological loop. According to Baddeley and Hitch, a central executive part of memory supervises or controls the flow of information to and from the three short-term systems.
https://youtu.be/pMMRE4Q2FGk
Video 5.5.2. Information Processing Model: Sensory, Working, and Long Term Memory explains the three-box model of memory.
Sensory Memory
In the Atkinson-Shiffrin model, stimuli from the environment are processed first in sensory memory: storage of brief sensory events, such as sights, sounds, and tastes. It is very brief storage, essentially long enough for the brain to register and start processing the information. Sensory memory can hold visual information for about half of a second and auditory information for a few seconds. Unlike other cognitive processes, it seems that sensory memory does not change from infancy (Siegler, 1998). However, without the ability to encode the information, it fades from sensory memory quickly (Papalia et al., 2008). As children and adolescence become more capable of encoding, they can take more advantage of the information available to them in the sensory memory.
We are constantly bombarded with sensory information. We cannot absorb all of it, or even most of it. Moreover, most of it has no impact on our lives. For example, what was your professor wearing the last class period? As long as the professor was dressed appropriately, it does not matter what she was wearing. Sensory information about sights, sounds, smells, and even textures, which we do not view as valuable information, we discard. If we view something as valuable, the information will move into our short-term memory system.
One study of sensory memory researched the significance of valuable information on short-term memory storage. J. R. Stroop discovered a memory phenomenon in the 1930s: you will name a color more easily if it appears printed in that color, which is called the Stroop effect. In other words, the word "red" will be named more quickly, regardless of the color the word appears in, than any word that is colored red. Try an experiment: name the colors of the words you are given in Figure 3.8.3. Do not read the words, but say the color the word is printed in. For example, upon seeing the word "yellow" in green print, you should say "green," not "yellow." This experiment is fun, but it is not as easy as it seems.
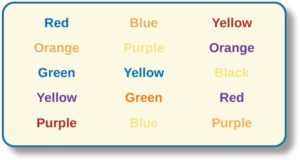
Figure 5.5.3. The Stroop effect describes why it is difficult for us to name a color when the word and the color of the word are different.
Short-Term (Working) Memory
Short-term memory (STM), also called working memory, is a temporary storage system that processes incoming sensory memory. Short-term memory is the bridge between information taken in through sensory memory and the more permanent storage of information in long-term memory. Information that is not moved along from short-term memory to long-term memory will be forgotten. Short-term memory is also called working memory because this is the system where the "work" of memory happens. If you are retrieving information from your long-term memory, you are moving it into your working memory, where you can think about that information.
Think of working memory as the information you have displayed on your computer screen—a document, a spreadsheet, or a web page. Then, the information in this memory system goes to long-term memory (you save it to your hard drive), or it is discarded (you delete a document or close a web browser). This step of rehearsal, the conscious repetition of information to be remembered, to move STM into long-term memory is called memory consolidation.
You may find yourself asking, "How much information can our memory handle at once?" To explore the capacity and duration of your short-term memory, have a partner read the strings of random numbers (Figure 3.8.4) out loud to you, beginning each string by saying, "Ready?" and ending each by saying, "Recall," at which point you should try to write down the string of numbers from memory.

Figure 5.5.4. Work through this series of numbers using the recall exercise explained above to determine the longest string of digits that you can store.
Note the longest string at which you got the series correct. For most people, this will be close to 7. Recall is somewhat better for random numbers than for random letters (Jacobs, 1887), and also often slightly better for information we hear (acoustic encoding) rather than see (visual encoding) (Anderson, 1969).
Short-term or working memory often requires conscious effort and adequate use of attention to function effectively. As you read earlier, children struggle with many aspects of attention, and this greatly diminishes their ability to juggle several pieces of information in memory consciously. The capacity of working memory is the amount of information someone can hold in consciousness is smaller in young children than in older children and adults. The typical 5-year-old can hold only a four-digit number active. The typical adult and teenager can hold a seven-digit number active in their short-term memory. The capacity of working memory expands during middle and late childhood, and research has suggested that both an increase in processing speed and the ability to inhibit irrelevant information from entering memory are contributing to the greater efficiency of working memory during this age (de Ribaupierre, 2001). Changes in myelination and synaptic pruning in the cortex are likely behind the increase in processing speed and ability to filter out irrelevant stimuli (Kail, McBride-chang, Ferrer, Cho, & Shu, 2013).
Short-term memory can only hold information for a short period of time, without rehearsal. For a typical adolescent or adult, storage lasts about 20-30 seconds. Older children and adults use mental strategies to aid their memory performance. For instance, simple rote rehearsal may be used to commit information to memory. Young children often do not rehearse unless reminded to do so, and when they do rehearse, they often fail to use clustering rehearsal. In clustering rehearsal, the person rehearses previous material while adding in additional information. If a list of words is read out loud to you, you are likely to rehearse each word as you hear it along with any previous words you were given. Young children will repeat each word they hear, but often fail to repeat the prior words in the list. In Schneider, Kron-Sperl, and Hunnerkopf's (2009) longitudinal study of 102 kindergarten children, the majority of children used no strategy to remember information, a finding that was consistent with previous research. As a result, their memory performance was reduced when compared to their abilities as they aged and started to use more effective memory strategies.
STM and Learning
Individuals differ in their memory abilities, and these differences predict academic performance (Peng et al., 2016). Children with learning disabilities in math and reading often have difficulties with working memory (Alloway, 2009). They may struggle with following the directions of an assignment. When a task calls for multiple steps, children with poor working memory may miss steps because they may lose track of where they are in the task. Adults working with such children may need to communicate: using more familiar vocabulary, using shorter sentences, repeating task instructions more frequently, and breaking more complex tasks into smaller, more manageable steps. Some studies have also shown that more intensive training of working memory strategies, such as chunking, aid in improving the capacity of working memory in children with poor working memory (Alloway, Bibile, & Lau, 2013).
Long-term Memory
Long-term memory (LTM) is the continuous storage of information. Unlike short-term memory, the storage capacity of LTM has no real limits. It encompasses all the things you can remember what happened more than just a few minutes ago to all of the things that you can remember what happened days, weeks, and years ago. In keeping with the computer analogy, the information in your LTM would be like the information you have saved on the hard drive. It is not there on your desktop (your short-term memory), but you can pull up this information when you want it, at least most of the time. Not all long-term memories are strong memories. Some memories can only be recalled through prompts. For example, you might easily recall a fact— "What is the capital of the United States?"—or a procedure—"How do you ride a bike?"—but you might struggle to recall the name of the restaurant you had dinner when you were on vacation in France last summer. A prompt, such as that the restaurant was named after its owner, who spoke to you about your shared interest in soccer, may help you recall the name of the restaurant.
Long-term memory is divided into two types: explicit and implicit (Figure 58.5). Understanding the different types is important because a person's age or particular types of brain trauma or disorders can leave certain types of LTM intact while having disastrous consequences for other types. Explicit memories, also called declarative memories, are those we consciously try to remember and recall. For example, if you are studying for your chemistry exam, the material you are learning will be part of your explicit memory. (Note: Sometimes, but not always, the terms explicit memory and declarative memory are used interchangeably.)
Implicit memories, also called non-declarative memories, are memories that are not part of our consciousness. They are memories formed from behaviors. Implicit memory is also called non-declarative memory.
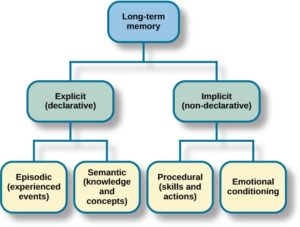
Figure 5.5.5. There are two components of long-term memory: explicit and implicit. Explicit memory includes episodic and semantic memory. Implicit memory includes procedural memory and things learned through conditioning.
Procedural memory is a type of implicit memory: it stores information about how to do things. It is the memory for skilled actions, such as how to brush your teeth, how to drive a car, how to swim the crawl (freestyle) stroke. If you are learning how to swim freestyle, you practice the stroke: how to move your arms, how to turn your head to alternate breathing from side to side, and how to kick your legs. You would practice this many times until you become good at it. Once you learn how to swim freestyle and your body knows how to move through the water, you will never forget how to swim freestyle, even if you do not swim for a couple of decades. Similarly, if you present an accomplished guitarist with a guitar, even if he has not played in a long time, he will still be able to play quite well.
Explicit or declarative memory has to do with the storage of facts and events we personally experienced. Explicit (declarative) memory has two parts: semantic memory and episodic memory. Semantic means having to do with language and knowledge about language. An example would be the question, "what does argumentative mean?" Stored in our semantic memory is knowledge about words, concepts, and language-based knowledge and facts. For example, answers to the following questions are stored in your semantic memory:
- Who was the first President of the United States?
- What is democracy?
- What is the longest river in the world?
Episodic memory is information about events we have personally experienced. The concept of episodic memory was first proposed about 40 years ago (Tulving, 1972). Since then, Tulving and others have looked at the scientific evidence and reformulated the theory. Currently, scientists believe that episodic memory is memory about happenings in particular places at particular times, the what, where, and when of an event (Tulving, 2002). It involves recollection of visual imagery as well as the feeling of familiarity (Hassabis & Maguire, 2007).
A component of episodic memory is autobiographical memory, or our personal narrative. Adolescents and adults rarely remember events from the first few years of life. We refer to this normal experience as infantile amnesia. In other words, we lack autobiographical memories from our experiences as an infant, toddler, and very young preschooler. Several factors contribute to the emergence of autobiographical memory, including brain maturation, improvements in language, opportunities to talk about experiences with parents and others, the development of theory of mind, and a representation of "self" (Nelson & Fivush, 2004). Two-year-olds do remember fragments of personal experiences, but these are rarely coherent accounts of past events (Nelson & Ross, 1980). Between 2 and 2 ½ years of age, children can provide more information about past experiences. However, these recollections require considerable prodding by adults (Nelson & Fivush, 2004). Over the next few years, children will form more detailed autobiographical memories and engage in more reflection of the past.
Retrieval
So you have worked hard to encode (via effortful processing) and store some important information for your upcoming final exam. How do you get that information back out of storage when you need it? The act of getting information out of memory storage and back into conscious awareness is known as retrieval. This process would be similar to finding and opening a paper you had previously saved on your computer's hard drive. Now it is back on your desktop, and you can work with it again. Our ability to retrieve information from long-term memory is vital to our everyday functioning. You must be able to retrieve information from memory in order to do everything from knowing how to brush your hair and teeth, to driving to work, to knowing how to perform your job once you get there.
https://youtu.be/aUmApJMfUTc
Video 5.5.1. Retrieval Cues discusses how cues prompt memory retrieval.
There are three ways to retrieve information from long-term memory storage systems: recall, recognition, and relearning. Recall is what we most often think about when we talk about memory retrieval: it means you can access information without cues. For example, you would use recall for an essay test. Recognition happens when you identify information that you have previously learned after re-encountering it. It involves a process of comparison. When you take a multiple-choice test, you are relying on recognition to help you choose the correct answer. Here is another example. Let us say you graduated from high school ten years ago, and you have returned to your hometown for your 10-year reunion. You may not be able to recall all of your classmates, but you recognize many of them based on their yearbook photos.
https://youtu.be/Uhyk2bRTguI
Video 5.5.2. Free Recall, Cued Recall, and Recognition discusses the various ways in which information can be retrieved from long term memory.
The third form of retrieval is relearning, and it is just as it sounds. It involves learning information that you previously learned. Whitney took Spanish in high school, but after high school, she did not have the opportunity to speak Spanish. Whitney is now 31, and her company has offered her an opportunity to work in their Mexico City office. In order to prepare herself, she enrolls in a Spanish course at the local community center. She is surprised at how quickly she can pick up the language after not speaking it for 13 years; this is an example of relearning.
Executive Functions
Changes in our information processing skills also involved changes in executive function. Executive function is generally understood to include three core components: working memory, shifting (also called cognitive flexibility), and inhibition. These components develop significantly during childhood and adolescence and are critical for academic, social, and emotional functioning.
Working Memory
As discussed earlier, working memory refers to the ability to temporarily hold and manipulate information in your mind. For example, if you're asked to solve 13 + 25 mentally, you might break the task into steps like this:
-
10 + 20 = 30
-
3 + 5 = 8
-
30 + 8 = 38
To arrive at the correct answer, you need to store intermediate results (30 and 8) while still actively processing the remaining steps. This illustrates how working memory allows us to hold onto partial information while performing mental operations.
Working memory is essential for nearly all everyday activities—from cooking and following instructions to reading comprehension and problem-solving. In the classroom, strong working memory supports learning across subjects, and children with higher working memory capacity often perform better academically.
Shifting
Shifting, or cognitive flexibility, refers to the ability to adapt your thinking and switch between different tasks, rules, or mental sets. For instance, moving from solving a math problem to reading a story requires a mental shift in focus and strategy.
Shifting is especially important in school settings, where students must frequently transition between subjects and activities. Even outside of academics, shifting is needed to navigate daily routines—for example, transitioning from a structured classroom environment to the more relaxed mindset of being at home. Strong shifting ability allows individuals to adapt more easily to changing situations and demands.
Inhibition
Inhibition is the ability to suppress automatic, impulsive, or irrelevant responses in favor of goal-directed behavior. A classic example is the Stroop task, where you're shown color words (e.g., the word "red" written in blue ink) and asked to name the ink color rather than reading the word. Doing so requires you to inhibit the automatic tendency to read the word and instead focus your attention on the color.
Figure 5.4.1. The Stroop effect is a task that requires inhibition
Inhibition is key to self-control and attention regulation. It helps children wait their turn, resist distractions, and follow rules—all of which are critical for successful learning and social interactions.
Development of Executive Function
These core components of executive function—working memory, shifting, and inhibition—begin to emerge in early childhood and continue to develop throughout childhood and adolescence. Like many other cognitive abilities, the development of executive function is shaped by both brain maturation—particularly in the prefrontal cortex—and environmental experiences. Research has shown that children raised in cognitively stimulating environments, with warm and responsive caregivers who use strategies such as scaffolding during problem-solving tasks, tend to develop stronger executive function skills (Fay-Stammbach, Hawes, & Meredith, 2014). For example, scaffolding behaviors have been found to be positively associated with cognitive flexibility at age two and inhibitory control at age four (Bibok, Carpendale, & Müller, 2009). These findings highlight the importance of both biological and social influences in supporting the development of self-regulation and higher-order thinking skills.
Executive Functions
Changes in our information processing skills also involved changes in executive function. Executive function is generally understood to include three core components: working memory, shifting (also called cognitive flexibility), and inhibition. These components develop significantly during childhood and adolescence and are critical for academic, social, and emotional functioning.
Working Memory
As discussed earlier, working memory refers to the ability to temporarily hold and manipulate information in your mind. For example, if you're asked to solve 13 + 25 mentally, you might break the task into steps like this:
-
10 + 20 = 30
-
3 + 5 = 8
-
30 + 8 = 38
To arrive at the correct answer, you need to store intermediate results (30 and 8) while still actively processing the remaining steps. This illustrates how working memory allows us to hold onto partial information while performing mental operations.
Working memory is essential for nearly all everyday activities—from cooking and following instructions to reading comprehension and problem-solving. In the classroom, strong working memory supports learning across subjects, and children with higher working memory capacity often perform better academically.
Shifting
Shifting, or cognitive flexibility, refers to the ability to adapt your thinking and switch between different tasks, rules, or mental sets. For instance, moving from solving a math problem to reading a story requires a mental shift in focus and strategy.
Shifting is especially important in school settings, where students must frequently transition between subjects and activities. Even outside of academics, shifting is needed to navigate daily routines—for example, transitioning from a structured classroom environment to the more relaxed mindset of being at home. Strong shifting ability allows individuals to adapt more easily to changing situations and demands.
Inhibition
Inhibition is the ability to suppress automatic, impulsive, or irrelevant responses in favor of goal-directed behavior. A classic example is the Stroop task, where you're shown color words (e.g., the word "red" written in blue ink) and asked to name the ink color rather than reading the word. Doing so requires you to inhibit the automatic tendency to read the word and instead focus your attention on the color.
Figure 5.6.1. The Stroop effect is a task that requires inhibition
Inhibition is key to self-control and attention regulation. It helps children wait their turn, resist distractions, and follow rules—all of which are critical for successful learning and social interactions.
Development of Executive Function
These core components of executive function—working memory, shifting, and inhibition—begin to emerge in early childhood and continue to develop throughout childhood and adolescence. Like many other cognitive abilities, the development of executive function is shaped by both brain maturation—particularly in the prefrontal cortex—and environmental experiences. Research has shown that children raised in cognitively stimulating environments, with warm and responsive caregivers who use strategies such as scaffolding during problem-solving tasks, tend to develop stronger executive function skills (Fay-Stammbach, Hawes, & Meredith, 2014). For example, scaffolding behaviors have been found to be positively associated with cognitive flexibility at age two and inhibitory control at age four (Bibok, Carpendale, & Müller, 2009). These findings highlight the importance of both biological and social influences in supporting the development of self-regulation and higher-order thinking skills.
Organization of Thinking
During middle childhood and adolescence, young people can learn and remember more due to improvements in the way they attend to and store information. As people learn more about the world, they develop more categories for concepts and learn more efficient strategies for storing and retrieving information. One significant reason is that they continue to have more experiences on which to tie new information. In other words, their knowledge base, knowledge in particular areas that makes learning new information easier, expands (Berger, 2014).
Inductive and Deductive Reasoning
Inductive reasoning emerges in childhood and is a type of reasoning that is sometimes characterized as "bottom-up- processing" in which specific observations, or specific comments from those in authority, may be used to draw general conclusions. However, in inductive reasoning, the veracity of the information that created the general conclusion does not guarantee the accuracy of that conclusion. For instance, a child who has only observed thunder on summer days may conclude that it only thunders in the summer. In contrast, deductive reasoning, sometimes called "top-down-processing," emerges in adolescence. This type of reasoning starts with some overarching principle and, based on this, propose specific conclusions. Deductive reasoning guarantees an accurate conclusion if the premises on which it is based are accurate.
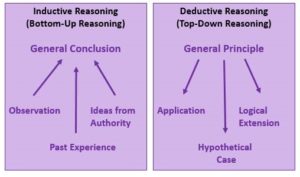
Figure 5.7.1. Models of inductive and deductive reasoning.
Intuitive versus Analytic Thinking
Cognitive psychologists often refer to intuitive and analytic thought as the Dual-Process Model, the notion that humans have two distinct networks for processing information (Albert & Steinberg, 2011). Intuitive thought is automatic, unconscious, and fast (Kahneman, 2011), and it is more experiential and emotional. In contrast, Analytic thought is deliberate, conscious, and rational. While these systems interact, they are distinct (Kuhn, 2013). Intuitive thought is easier and more commonly used in everyday life. It is also more commonly used by children and teens than by adults (Klaczynski, 2001). The quickness of adolescent thought, along with the maturation of the limbic system, may make teens more prone to emotional, intuitive thinking than adults.
Critical Thinking
There is a debate in U.S. education as to whether schools should teach students what to think or how to think. Critical thinking, or a detailed examination of beliefs, courses of action, and evidence, involves teaching children how to think. The purpose of critical thinking is to evaluate information in ways that help us make informed decisions. Critical thinking involves better understanding a problem through gathering, evaluating, and selecting information, and also by considering many possible solutions. Ennis (1987) identified several skills useful in critical thinking. These include: Analyzing arguments, clarifying information, judging the credibility of a source, making value judgments, and deciding on an action. Metacognition is essential to critical thinking because it allows us to reflect on the information as we make decisions.
Metacognition
As children mature through middle and late childhood and into adolescence, they have a better understanding of how well they are performing a task and the level of difficulty of a task. As they become more realistic about their abilities, they can adapt studying strategies to meet those needs. Young children spend as much time on an unimportant aspect of a problem as they do on the main point, while older children start to learn to prioritize and gauge what is significant and what is not. As a result, they develop metacognition. Metacognition refers to the knowledge we have about our thinking and our ability to use this awareness to regulate our cognitive processes.
Bjorklund (2005) describes a developmental progression in the acquisition and use of memory strategies. Such strategies are often lacking in younger children but increase in frequency as children progress through elementary school. Examples of memory strategies include rehearsing information you wish to recall, visualizing and organizing information, creating rhymes, such as "i" before "e" except after "c," or inventing acronyms, such as "ROYGBIV" to remember the colors of the rainbow. Schneider, Kron-Sperl, and hünnerkopf (2009) reported a steady increase in the use of memory strategies from ages six to ten in their longitudinal study (see table 5.7.1). Moreover, by age ten, many children were using two or more memory strategies to help them recall information. Schneider and colleagues found that there were considerable individual differences at each age in the use of strategies and that children who utilized more strategies had better memory performance than their same-aged peers.
Table 5.7.1. Percentage of children who did not use any memory strategies by age.
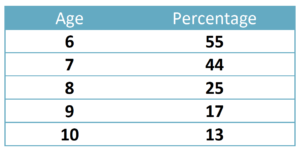
A person may experience three deficiencies in their use of memory strategies. A mediation deficiency occurs when a person does not grasp the strategy being taught, and thus, does not benefit from its use. If you do not understand why using an acronym might be helpful, or how to create an acronym, the strategy is not likely to help you. In a production deficiency, the person does not spontaneously use a memory strategy and has to be prompted to do so. In this case, the person knows the strategy and is more than capable of using it, but they fail to "produce" the strategy on their own. For example, a child might know how to make a list but may fail to do this to help them remember what to bring on a family vacation. A utilization deficiency refers to a person using an appropriate strategy, but it fails to aid their performance. Utilization deficiency is common in the early stages of learning a new memory strategy (Schneider & Pressley, 1997; miller, 2000). Until the use of the strategy becomes automatic, it may slow down the learning process, as space is taken up in memory by the strategy itself. Initially, children may get frustrated because their memory performance may seem worse when they try to use the new strategy. Once children become more adept at using the strategy, their memory performance will improve. Sodian and Schneider (1999) found that new memory strategies acquired before age 8 often show utilization deficiencies, with there being a gradual improvement in the child's use of the strategy. In contrast, strategies acquired after this age often followed an "all-or-nothing" principle in which improvement was not gradual, but abrupt.
Memory is an information processing system; therefore, we often compare it to a computer. Memory is the set of processes used to encode, store, and retrieve information over different periods of time.
Figure 5.5.1. Encoding involves the input of information into the memory system. Storage is the retention of encoded information. Retrieval, or getting the information out of memory and back into awareness, is the third function.
Encoding
We get information into our brains through a process called encoding, which is the input of information into the memory system. Once we receive sensory information from the environment, our brains label or code it. We organize the information with other similar information and connect new concepts to existing concepts. Encoding information occurs through automatic processing and effortful processing.
If someone asks you what you ate for lunch today, more than likely, you could recall this information quite easily. This is known as automatic processing, or the encoding of details like time, space, frequency, and the meaning of words. Automatic processing is usually done without any conscious awareness. Recalling the last time you studied for a test is another example of automatic processing. However, what about the actual test material that you studied? It probably required a lot of work and attention on your part in order to encode that information. This is known as effortful processing.
There are three types of encoding. The encoding of words and their meaning is known as semantic encoding. It was first demonstrated by William Bousfield (1935) in an experiment in which he asked people to memorize words. The 60 words were divided into 4 categories of meaning, although the participants did not know this because the words were randomly presented. When they were asked to remember the words, they tended to recall them in categories, showing that they paid attention to the meanings of the words as they learned them.
Visual encoding is the encoding of images, and acoustic encoding is the encoding of sounds, words in particular. To see how visual encoding works, read over this list of words: car, level, dog, truth, book, value. If you were asked later to recall the words from this list, which ones do you think you'd most likely remember? You would probably have an easier time recalling the words car, dog, and book, and a more difficult time recalling the words level, truth, and value. Why is this? Because you can recall images (mental pictures) more easily than words alone. When you read the words car, dog, and book, you created images of these things in your mind. These are concrete, high-imagery words. On the other hand, abstract words like level, truth, and value are low-imagery words. High-imagery words are encoded both visually and semantically (Paivio, 1986), thus building a more reliable memory.
Now let us turn our attention to acoustic encoding. You are driving in your car, and a song comes on the radio that you have not heard in at least ten years, but you sing along, recalling every word. In the United States, children often learn the alphabet through song, and they learn the number of days in each month through rhyme: "Thirty days hath September, / April, June, and November; / All the rest have thirty-one, / Save February, with twenty-eight days clear, / And twenty-nine each leap year." These lessons are easy to remember because of acoustic encoding. We encode the sounds the words make. This is one of the reasons why much of what we teach young children is done through song, rhyme, and rhythm.
Which of the three types of encoding do you think would give you the best memory of verbal information? Some years ago, psychologists Fergus Craik and Endel Tulving (1975) conducted a series of experiments to find out. Participants were given words along with questions about them. The questions required the participants to process the words at one of the three levels. The visual processing questions included such things as asking the participants about the font of the letters. The acoustic processing questions asked the participants about the sound or rhyming of the words, and the semantic processing questions asked the participants about the meaning of the words. After participants were presented with the words and questions, they were given an unexpected recall or recognition task.
Words that had been encoded semantically were better remembered than those encoded visually or acoustically. Semantic encoding involves a deeper level of processing than shallower visual or acoustic encoding. Craik and Tulving concluded that we process verbal information best through semantic encoding, especially if we apply what is called the self-reference effect. The self-reference effect is the tendency for an individual to have a better memory for information that relates to oneself in comparison to material that has less personal relevance (Rogers, Kuiper & Kirker, 1977). Could semantic encoding be beneficial to you as you attempt to memorize the concepts in this chapter?
https://youtu.be/mlrOJgyPySw
Video 5.5.1. Encoding Strategies discusses various encoding techniques that help us store information in memory.
Storage
Once the information has been encoded, we have to retain it somehow. Our brains take the encoded information and place it in storage. Storage is the creation of a permanent record of information.
In order for a memory to go into storage (i.e., long-term memory), it has to pass through three distinct stages: Sensory Memory, Short-Term Memory, and finally, Long-Term Memory. These stages were first proposed by Richard Atkinson and Richard Shiffrin (1968). Their model of human memory, called Atkinson-Shiffrin (A-S) or three-box model, is based on the belief that we process memories in the same way that a computer processes information.
Figure 5.5.2. According to the Atkinson-Shiffrin model of memory, information passes through three distinct stages in order for it to be stored in long-term memory.
The three-box is just one model of memory. Others, such as Hitch and Baddeley (1976), have proposed a model where short-term memory itself has different forms. In this model, storing memories in short-term memory is like opening different files on a computer and adding information. The type of short-term memory (or computer file) depends on the type of information received. There are memories in visual-spatial form, as well as memories of spoken or written material, and they are stored in three short-term systems: a visuospatial sketchpad, an episodic buffer, and a phonological loop. According to Baddeley and Hitch, a central executive part of memory supervises or controls the flow of information to and from the three short-term systems.
https://youtu.be/pMMRE4Q2FGk
Video 5.5.2. Information Processing Model: Sensory, Working, and Long Term Memory explains the three-box model of memory.
Sensory Memory
In the Atkinson-Shiffrin model, stimuli from the environment are processed first in sensory memory: storage of brief sensory events, such as sights, sounds, and tastes. It is very brief storage, essentially long enough for the brain to register and start processing the information. Sensory memory can hold visual information for about half of a second and auditory information for a few seconds. Unlike other cognitive processes, it seems that sensory memory does not change from infancy (Siegler, 1998). However, without the ability to encode the information, it fades from sensory memory quickly (Papalia et al., 2008). As children and adolescence become more capable of encoding, they can take more advantage of the information available to them in the sensory memory.
We are constantly bombarded with sensory information. We cannot absorb all of it, or even most of it. Moreover, most of it has no impact on our lives. For example, what was your professor wearing the last class period? As long as the professor was dressed appropriately, it does not matter what she was wearing. Sensory information about sights, sounds, smells, and even textures, which we do not view as valuable information, we discard. If we view something as valuable, the information will move into our short-term memory system.
One study of sensory memory researched the significance of valuable information on short-term memory storage. J. R. Stroop discovered a memory phenomenon in the 1930s: you will name a color more easily if it appears printed in that color, which is called the Stroop effect. In other words, the word "red" will be named more quickly, regardless of the color the word appears in, than any word that is colored red. Try an experiment: name the colors of the words you are given in Figure 3.8.3. Do not read the words, but say the color the word is printed in. For example, upon seeing the word "yellow" in green print, you should say "green," not "yellow." This experiment is fun, but it is not as easy as it seems.
Figure 5.5.3. The Stroop effect describes why it is difficult for us to name a color when the word and the color of the word are different.
Short-Term (Working) Memory
Short-term memory (STM), also called working memory, is a temporary storage system that processes incoming sensory memory. Short-term memory is the bridge between information taken in through sensory memory and the more permanent storage of information in long-term memory. Information that is not moved along from short-term memory to long-term memory will be forgotten. Short-term memory is also called working memory because this is the system where the "work" of memory happens. If you are retrieving information from your long-term memory, you are moving it into your working memory, where you can think about that information.
Think of working memory as the information you have displayed on your computer screen—a document, a spreadsheet, or a web page. Then, the information in this memory system goes to long-term memory (you save it to your hard drive), or it is discarded (you delete a document or close a web browser). This step of rehearsal, the conscious repetition of information to be remembered, to move STM into long-term memory is called memory consolidation.
You may find yourself asking, "How much information can our memory handle at once?" To explore the capacity and duration of your short-term memory, have a partner read the strings of random numbers (Figure 3.8.4) out loud to you, beginning each string by saying, "Ready?" and ending each by saying, "Recall," at which point you should try to write down the string of numbers from memory.
Figure 5.5.4. Work through this series of numbers using the recall exercise explained above to determine the longest string of digits that you can store.
Note the longest string at which you got the series correct. For most people, this will be close to 7. Recall is somewhat better for random numbers than for random letters (Jacobs, 1887), and also often slightly better for information we hear (acoustic encoding) rather than see (visual encoding) (Anderson, 1969).
Short-term or working memory often requires conscious effort and adequate use of attention to function effectively. As you read earlier, children struggle with many aspects of attention, and this greatly diminishes their ability to juggle several pieces of information in memory consciously. The capacity of working memory is the amount of information someone can hold in consciousness is smaller in young children than in older children and adults. The typical 5-year-old can hold only a four-digit number active. The typical adult and teenager can hold a seven-digit number active in their short-term memory. The capacity of working memory expands during middle and late childhood, and research has suggested that both an increase in processing speed and the ability to inhibit irrelevant information from entering memory are contributing to the greater efficiency of working memory during this age (de Ribaupierre, 2001). Changes in myelination and synaptic pruning in the cortex are likely behind the increase in processing speed and ability to filter out irrelevant stimuli (Kail, McBride-chang, Ferrer, Cho, & Shu, 2013).
Short-term memory can only hold information for a short period of time, without rehearsal. For a typical adolescent or adult, storage lasts about 20-30 seconds. Older children and adults use mental strategies to aid their memory performance. For instance, simple rote rehearsal may be used to commit information to memory. Young children often do not rehearse unless reminded to do so, and when they do rehearse, they often fail to use clustering rehearsal. In clustering rehearsal, the person rehearses previous material while adding in additional information. If a list of words is read out loud to you, you are likely to rehearse each word as you hear it along with any previous words you were given. Young children will repeat each word they hear, but often fail to repeat the prior words in the list. In Schneider, Kron-Sperl, and Hunnerkopf's (2009) longitudinal study of 102 kindergarten children, the majority of children used no strategy to remember information, a finding that was consistent with previous research. As a result, their memory performance was reduced when compared to their abilities as they aged and started to use more effective memory strategies.
STM and Learning
Individuals differ in their memory abilities, and these differences predict academic performance (Peng et al., 2016). Children with learning disabilities in math and reading often have difficulties with working memory (Alloway, 2009). They may struggle with following the directions of an assignment. When a task calls for multiple steps, children with poor working memory may miss steps because they may lose track of where they are in the task. Adults working with such children may need to communicate: using more familiar vocabulary, using shorter sentences, repeating task instructions more frequently, and breaking more complex tasks into smaller, more manageable steps. Some studies have also shown that more intensive training of working memory strategies, such as chunking, aid in improving the capacity of working memory in children with poor working memory (Alloway, Bibile, & Lau, 2013).
Long-term Memory
Long-term memory (LTM) is the continuous storage of information. Unlike short-term memory, the storage capacity of LTM has no real limits. It encompasses all the things you can remember what happened more than just a few minutes ago to all of the things that you can remember what happened days, weeks, and years ago. In keeping with the computer analogy, the information in your LTM would be like the information you have saved on the hard drive. It is not there on your desktop (your short-term memory), but you can pull up this information when you want it, at least most of the time. Not all long-term memories are strong memories. Some memories can only be recalled through prompts. For example, you might easily recall a fact— "What is the capital of the United States?"—or a procedure—"How do you ride a bike?"—but you might struggle to recall the name of the restaurant you had dinner when you were on vacation in France last summer. A prompt, such as that the restaurant was named after its owner, who spoke to you about your shared interest in soccer, may help you recall the name of the restaurant.
Long-term memory is divided into two types: explicit and implicit (Figure 5.5.5). Understanding the different types is important because a person's age or particular types of brain trauma or disorders can leave certain types of LTM intact while having disastrous consequences for other types. Explicit memories, also called declarative memories, are those we consciously try to remember and recall. For example, if you are studying for your chemistry exam, the material you are learning will be part of your explicit memory. (Note: Sometimes, but not always, the terms explicit memory and declarative memory are used interchangeably.)
Implicit memories, also called non-declarative memories, are memories that are not part of our consciousness. They are memories formed from behaviors. Implicit memory is also called non-declarative memory.
Figure 5.5.5. There are two components of long-term memory: explicit and implicit. Explicit memory includes episodic and semantic memory. Implicit memory includes procedural memory and things learned through conditioning.
Procedural memory is a type of implicit memory: it stores information about how to do things. It is the memory for skilled actions, such as how to brush your teeth, how to drive a car, how to swim the crawl (freestyle) stroke. If you are learning how to swim freestyle, you practice the stroke: how to move your arms, how to turn your head to alternate breathing from side to side, and how to kick your legs. You would practice this many times until you become good at it. Once you learn how to swim freestyle and your body knows how to move through the water, you will never forget how to swim freestyle, even if you do not swim for a couple of decades. Similarly, if you present an accomplished guitarist with a guitar, even if he has not played in a long time, he will still be able to play quite well.
Explicit or declarative memory has to do with the storage of facts and events we personally experienced. Explicit (declarative) memory has two parts: semantic memory and episodic memory. Semantic means having to do with language and knowledge about language. An example would be the question, "what does argumentative mean?" Stored in our semantic memory is knowledge about words, concepts, and language-based knowledge and facts. For example, answers to the following questions are stored in your semantic memory:
- Who was the first President of the United States?
- What is democracy?
- What is the longest river in the world?
Episodic memory is information about events we have personally experienced. The concept of episodic memory was first proposed about 40 years ago (Tulving, 1972). Since then, Tulving and others have looked at the scientific evidence and reformulated the theory. Currently, scientists believe that episodic memory is memory about happenings in particular places at particular times, the what, where, and when of an event (Tulving, 2002). It involves recollection of visual imagery as well as the feeling of familiarity (Hassabis & Maguire, 2007).
A component of episodic memory is autobiographical memory, or our personal narrative. Adolescents and adults rarely remember events from the first few years of life. We refer to this normal experience as infantile amnesia. In other words, we lack autobiographical memories from our experiences as an infant, toddler, and very young preschooler. Several factors contribute to the emergence of autobiographical memory, including brain maturation, improvements in language, opportunities to talk about experiences with parents and others, the development of theory of mind, and a representation of "self" (Nelson & Fivush, 2004). Two-year-olds do remember fragments of personal experiences, but these are rarely coherent accounts of past events (Nelson & Ross, 1980). Between 2 and 2 ½ years of age, children can provide more information about past experiences. However, these recollections require considerable prodding by adults (Nelson & Fivush, 2004). Over the next few years, children will form more detailed autobiographical memories and engage in more reflection of the past.
Retrieval
So you have worked hard to encode (via effortful processing) and store some important information for your upcoming final exam. How do you get that information back out of storage when you need it? The act of getting information out of memory storage and back into conscious awareness is known as retrieval. This process would be similar to finding and opening a paper you had previously saved on your computer's hard drive. Now it is back on your desktop, and you can work with it again. Our ability to retrieve information from long-term memory is vital to our everyday functioning. You must be able to retrieve information from memory in order to do everything from knowing how to brush your hair and teeth, to driving to work, to knowing how to perform your job once you get there.
https://youtu.be/aUmApJMfUTc
Video 5.5.1. Retrieval Cues discusses how cues prompt memory retrieval.
There are three ways to retrieve information from long-term memory storage systems: recall, recognition, and relearning. Recall is what we most often think about when we talk about memory retrieval: it means you can access information without cues. For example, you would use recall for an essay test. Recognition happens when you identify information that you have previously learned after re-encountering it. It involves a process of comparison. When you take a multiple-choice test, you are relying on recognition to help you choose the correct answer. Here is another example. Let us say you graduated from high school ten years ago, and you have returned to your hometown for your 10-year reunion. You may not be able to recall all of your classmates, but you recognize many of them based on their yearbook photos.
https://youtu.be/Uhyk2bRTguI
Video 5.5.2. Free Recall, Cued Recall, and Recognition discusses the various ways in which information can be retrieved from long term memory.
The third form of retrieval is relearning, and it is just as it sounds. It involves learning information that you previously learned. Whitney took Spanish in high school, but after high school, she did not have the opportunity to speak Spanish. Whitney is now 31, and her company has offered her an opportunity to work in their Mexico City office. In order to prepare herself, she enrolls in a Spanish course at the local community center. She is surprised at how quickly she can pick up the language after not speaking it for 13 years; this is an example of relearning.
Alloway, T. P. (2009). Working memory, but not IQ, predicts subsequent learning in children with learning difficulties. European journal of psychological assessment, 25(2), 92-98.
Alloway, T. P., Bibile, V., & Lau, G. (2013). Computerized working memory training: Can it lead to gains in cognitive skills in students?. Computers in Human Behavior, 29(3), 632-638.
Anderson, S. R. (1969). West Scandinavian vowel systems and the ordering of phonological rules (Doctoral dissertation, Massachusetts Institute of Technology).
Atkinson, R. C., & Shiffrin, R. M. (1968). Human memory: A proposed system and its control processes. In Psychology of learning and motivation (Vol. 2, pp. 89-195). Academic press.
Bibok, M. B., Carpendale, J. I., & Müller, U. (2009). Parental scaffolding and the development of executive function. New directions for child and adolescent development, 2009(123), 17-34.
Case, R., Okamoto, Y., Griffin, S., McKeough, A., Bleiker, C., Henderson, B., ... & Keating, D. P. (1996). The role of central conceptual structures in the development of children's thought. Monographs of the society for research in child development, i-295.
Carlson, S. M., Zelazo, P. D., & Faja, S. (2013). Executive function.
Collet, C., Clarion, A., Morel, M., Chapon, A., & Petit, C. (2009). Physiological and behavioural changes associated to the management of secondary tasks while driving. Applied ergonomics, 40(6), 1041-1046.
Crain, W. (2007). Homework and the Freedom to Think. Reading Against Democracy: The Broken Promises of Reading Instruction, 20(4), 30.
de Ribaupierre, A. (2001). Working memory and attentional processes across the lifespan. Lifespan development of human memory, 59-80.
Elkind, D. (1967). Egocentrism in adolescence. Child development, 1025-1034.
Fay‐Stammbach, T., Hawes, D. J., & Meredith, P. (2014). Parenting influences on executive function in early childhood: A review. Child development perspectives, 8(4), 258-264.
Kail, R. V., McBride‐Chang, C., Ferrer, E., Cho, J. R., & Shu, H. (2013). Cultural differences in the development of processing speed. Developmental science, 16(3), 476-483.
Guy, J., Rogers, M., & Cornish, K. (2013). Age-related changes in visual and auditory sustained attention in preschool-aged children. Child Neuropsychology, 19(6), 601-614.
Hassabis, D., & Maguire, E. A. (2007). Deconstructing episodic memory with construction. Trends in cognitive sciences, 11(7), 299-306.
Herrmann, E., Misch, A., Hernandez‐Lloreda, V., & Tomasello, M. (2015). Uniquely human self‐control begins at school age. Developmental science, 18(6), 979-993.
Herrmann, E., & Tomasello, M. (2015). Focusing and shifting attention in human children (Homo sapiens) and chimpanzees (Pan troglodytes). Journal of Comparative Psychology, 129(3), 268.
Hitch, G. J., & Baddeley, A. D. (1976). Verbal reasoning and working memory. The Quarterly Journal of Experimental Psychology, 28(4), 603-621.
Jones, P. R., Moore, D. R., & Amitay, S. (2015). Development of auditory selective attention: why children struggle to hear in noisy environments. Developmental psychology, 51(3), 353.
Klaczynski, P. A., & Felmban, W. S. (2014). Adolescent development: Heuristics, biases, and individual differences. The developmental psychology of reasoning and decision‐making, 84-112.
Kuhn, D., Zillmer, N., Crowell, A., & Zavala, J. (2013). Developing norms of argumentation: Metacognitive, epistemological, and social dimensions of developing argumentive competence. Cognition and Instruction, 31(4), 456-496.
Matlin, M. W. (2013). Margaret W. Matlin. In Models of Achievement (pp. 239-254). Psychology Press.
Nelson, K., & Fivush, R. (2004). The emergence of autobiographical memory: a social cultural developmental theory. Psychological review, 111(2), 486.
Peng, P., Namkung, J., Barnes, M., & Sun, C. (2016). A meta-analysis of mathematics and working memory: Moderating effects of working memory domain, type of mathematics skill, and sample characteristics. Journal of Educational Psychology, 108(4), 455.
Piaget, J., & Inhelder, B. (2014). Intellectual operations and their development. In Experimental Psychology Its Scope and Method: Volume VII (Psychology Revivals) (pp. 144-205). Psychology Press.
Porporino, M., Iarocci, G., Shore, D. I., & Burack, J. A. (2004). A developmental change in selective attention and global form perception. International Journal of Behavioral Development, 28(4), 358-364.
Posner, M. I., & Rothbart, M. K. (2007). Research on attention networks as a model for the integration of psychological science. Annu. Rev. Psychol., 58(1), 1-23.
Raichle, M. E. (2015). The brain's default mode network. Annual review of neuroscience, 38(1), 433-447.
Rueda, M. R., Rothbart, M. K., McCandliss, B. D., Saccomanno, L., & Posner, M. I. (2005). Training, maturation, and genetic influences on the development of executive attention. Proceedings of the National Academy of Sciences, 102(41), 14931-14936.
Salvucci, D. D., & Taatgen, N. A. (2008). Threaded cognition: an integrated theory of concurrent multitasking. Psychological review, 115(1), 101.
Schwartz, P. D., Maynard, A. M., & Uzelac, S. M. (2008). Adolescent egocentrism: a contemporary view. Adolescence, 43(171), 441-449.
Siegler, R. S. (1998). Emerging minds: The process of change in children's thinking. Oxford University Press.
Sinnott, J. (1998). The development of logic in adulthood: Postformal thought and its applications. Springer Science & Business Media.
Sternberg, R. J. (2012). The assessment of creativity: An investment-based approach. Creativity research journal, 24(1), 3-12.
Strayer, D. L., & Drews, F. A. (2007). Cell-phone–induced driver distraction. Current Directions in Psychological Science, 16(3), 128-131.
Tulving, E. (1972). Episodic and semantic memory. Organization of memory, 1(381-403), 1.
Tulving, E. (2002). Episodic memory: From mind to brain. Annual review of psychology, 53(1), 1-25.
Vakil, E., Greenstein, Y., & Blachstein, H. (2010). Normative data for composite scores for children and adults derived from the Rey Auditory Verbal Learning Test. The Clinical Neuropsychologist, 24(4), 662-677.
Vygotsky, L. S. (1962). Language and thought (pp. 11193-000). Cambridge, MA: MIT Press.
Organization of Thinking
During middle childhood and adolescence, young people can learn and remember more due to improvements in the way they attend to and store information. As people learn more about the world, they develop more categories for concepts and learn more efficient strategies for storing and retrieving information. One significant reason is that they continue to have more experiences on which to tie new information. In other words, their knowledge base, knowledge in particular areas that makes learning new information easier, expands (Berger, 2014).
Inductive and Deductive Reasoning
Inductive reasoning emerges in childhood and is a type of reasoning that is sometimes characterized as "bottom-up- processing" in which specific observations, or specific comments from those in authority, may be used to draw general conclusions. However, in inductive reasoning, the veracity of the information that created the general conclusion does not guarantee the accuracy of that conclusion. For instance, a child who has only observed thunder on summer days may conclude that it only thunders in the summer. In contrast, deductive reasoning, sometimes called "top-down-processing," emerges in adolescence. This type of reasoning starts with some overarching principle and, based on this, propose specific conclusions. Deductive reasoning guarantees an accurate conclusion if the premises on which it is based are accurate.
Figure 5.7.1. Models of inductive and deductive reasoning.
Intuitive versus Analytic Thinking
Cognitive psychologists often refer to intuitive and analytic thought as the Dual-Process Model, the notion that humans have two distinct networks for processing information (Albert & Steinberg, 2011). Intuitive thought is automatic, unconscious, and fast (Kahneman, 2011), and it is more experiential and emotional. In contrast, Analytic thought is deliberate, conscious, and rational. While these systems interact, they are distinct (Kuhn, 2013). Intuitive thought is easier and more commonly used in everyday life. It is also more commonly used by children and teens than by adults (Klaczynski, 2001). The quickness of adolescent thought, along with the maturation of the limbic system, may make teens more prone to emotional, intuitive thinking than adults.
Critical Thinking
There is a debate in U.S. education as to whether schools should teach students what to think or how to think. Critical thinking, or a detailed examination of beliefs, courses of action, and evidence, involves teaching children how to think. The purpose of critical thinking is to evaluate information in ways that help us make informed decisions. Critical thinking involves better understanding a problem through gathering, evaluating, and selecting information, and also by considering many possible solutions. Ennis (1987) identified several skills useful in critical thinking. These include: Analyzing arguments, clarifying information, judging the credibility of a source, making value judgments, and deciding on an action. Metacognition is essential to critical thinking because it allows us to reflect on the information as we make decisions.
Metacognition
As children mature through middle and late childhood and into adolescence, they have a better understanding of how well they are performing a task and the level of difficulty of a task. As they become more realistic about their abilities, they can adapt studying strategies to meet those needs. Young children spend as much time on an unimportant aspect of a problem as they do on the main point, while older children start to learn to prioritize and gauge what is significant and what is not. As a result, they develop metacognition. Metacognition refers to the knowledge we have about our thinking and our ability to use this awareness to regulate our cognitive processes.
Bjorklund (2005) describes a developmental progression in the acquisition and use of memory strategies. Such strategies are often lacking in younger children but increase in frequency as children progress through elementary school. Examples of memory strategies include rehearsing information you wish to recall, visualizing and organizing information, creating rhymes, such as "i" before "e" except after "c," or inventing acronyms, such as "ROYGBIV" to remember the colors of the rainbow. Schneider, Kron-Sperl, and hünnerkopf (2009) reported a steady increase in the use of memory strategies from ages six to ten in their longitudinal study (see table 5.7.1). Moreover, by age ten, many children were using two or more memory strategies to help them recall information. Schneider and colleagues found that there were considerable individual differences at each age in the use of strategies and that children who utilized more strategies had better memory performance than their same-aged peers.
Table 5.7.1. Percentage of children who did not use any memory strategies by age.
A person may experience three deficiencies in their use of memory strategies. A mediation deficiency occurs when a person does not grasp the strategy being taught, and thus, does not benefit from its use. If you do not understand why using an acronym might be helpful, or how to create an acronym, the strategy is not likely to help you. In a production deficiency, the person does not spontaneously use a memory strategy and has to be prompted to do so. In this case, the person knows the strategy and is more than capable of using it, but they fail to "produce" the strategy on their own. For example, a child might know how to make a list but may fail to do this to help them remember what to bring on a family vacation. A utilization deficiency refers to a person using an appropriate strategy, but it fails to aid their performance. Utilization deficiency is common in the early stages of learning a new memory strategy. Until the use of the strategy becomes automatic, it may slow down the learning process, as space is taken up in memory by the strategy itself. Initially, children may get frustrated because their memory performance may seem worse when they try to use the new strategy. Once children become more adept at using the strategy, their memory performance will improve. Sodian and Schneider (1999) found that new memory strategies acquired before age 8 often show utilization deficiencies, with there being a gradual improvement in the child's use of the strategy. In contrast, strategies acquired after this age often followed an "all-or-nothing" principle in which improvement was not gradual, but abrupt.
For nearly a century, educators and psychologists have debated the nature of intelligence, and more specifically whether intelligence is just one broad ability or can take more than one form. Many classical definitions of the concept have tended to define intelligence as a single broad ability that allows a person to solve or complete many sorts of tasks, or at least many academic tasks like reading, knowledge of vocabulary, and the solving of logical problems (Garlick, 2002). Other psychologists believe that instead of a single factor, intelligence is a collection of distinct abilities. Still, other psychologists believe that intelligence should be defined in more practical terms. We'll review three perspectives on intelligence, Spearman's g, Sternberg's Triarchic Theory of Intelligence, and Gardner's Frame of Mind. Understanding theories of intelligence will help us understand variations in students' intellectual abilities.
British psychologist Charles Spearman believed intelligence consisted of one general factor, called g, which could be measured and compared among individuals. Spearman focused on the commonalities among various intellectual abilities and deemphasized what made each unique. There is research evidence of such a global ability, and the idea of general intelligence often fits with society’s everyday beliefs about intelligence. Partly for these reasons, an entire mini-industry has grown up around publishing tests of intelligence, academic ability, and academic achievement. Since these tests affect the work of teachers, I return to discussing them later in this book.
https://youtu.be/F9n3hLnwwc0
Video 5.8.1. Intelligence explains the different definitions of intelligence and the nature/nurture debate in the context of intelligence.
Theories of Intelligence
Psychologists have long debated how to best conceptualize and measure intelligence (Sternberg, 2003). These questions include how many types of intelligence there are, the role of nature versus nurture in intelligence, how intelligence is represented in the brain, and the meaning of group differences in intelligence.
https://youtu.be/oaJ01Ex7DLw
Video 5.8.2. Theories of Intelligence reviews a few of the different theoretical views of intelligence.
General Intelligence Factor ("g")
From 1904-1905 the French psychologist Alfred Binet (1857–1914) and his colleague Théodore Simon (1872–1961) began working on behalf of the French government to develop a measure that would identify children who would not be successful with the regular school curriculum. The goal was to help teachers better educate these students (Aiken, 1996). Binet and Simon developed what most psychologists today regard as the first intelligence test, which consisted of a wide variety of questions that included the ability to name objects, define words, draw pictures, complete sentences, compare items, and construct sentences.
Binet and Simon (Binet, Simon, & Town, 1915; Siegler, 1992) believed that the questions they asked the children all assessed the basic abilities to understand, reason, and make judgments. It turned out that the correlations among these different types of measures were, in fact, all positive; that is, students who got one item correct were more likely to also get other items correct, even though the questions themselves were very different.
On the basis of these results, the psychologist Charles Spearman (1863–1945) hypothesized that there must be a single underlying construct that all of these items measure. He called the construct that the different abilities and skills measured on intelligence tests have in common the general intelligence factor (g). Virtually all psychologists now believe that there is a generalized intelligence factor, "g," that relates to abstract thinking and that includes the abilities to acquire knowledge, to reason abstractly, to adapt to novel situations, and to benefit from instruction and experience (Gottfredson, 1997; Sternberg, 2003). People with higher general intelligence learn faster.
Soon after Binet and Simon introduced their test, the American psychologist Lewis Terman at Stanford University (1877–1956) developed an American version of Binet's test that became known as the Stanford- Binet intelligence test. The Stanford-Binet is a measure of general intelligence made up of a wide variety of tasks, including vocabulary, memory for pictures, naming of familiar objects, repeating sentences, and following commands.
Sternberg's Triarchic theory
Although there is general agreement among psychologists that "g" exists, there is also evidence for specific intelligence "s," a measure of specific skills in narrow domains. One empirical result in support of the idea of "s" comes from intelligence tests themselves. Although the different types of questions do correlate with each other, some items correlate more highly with each other than do other items; they form clusters or clumps of intelligences.
One advocate of the idea of multiple intelligences is the psychologist Robert Sternberg. Sternberg has proposed a Triarchic (three-part) Theory of Intelligence that proposes that people may display more or less analytical intelligence, creative intelligence, and practical intelligence. Sternberg (1985, 2003) argued that traditional intelligence tests assess analytical intelligence, academic problem solving and performing calculations, but that they do not typically assess creative intelligence, the ability to adapt to new situations and create new ideas, and/or practical intelligence, the ability to demonstrate common sense and street- smarts.
As Sternberg proposed, research has found that creativity is not highly correlated with analytical intelligence (Furnham & Bakhtiar, 2008), and exceptionally creative scientists, artists, mathematicians, and engineers do not score higher on intelligence than do their less creative peers (Simonton, 2000). Furthermore, the brain areas that are associated with convergent thinking, thinking that is directed toward finding the correct answer to a given problem, are different from those associated with divergent thinking, the ability to generate many different ideas or solutions to a single problem (Tarasova, Volf, & Razoumnikova, 2010). On the other hand, being creative often takes some of the basic abilities measured by "g," including the abilities to learn from experience, to remember information, and to think abstractly (Bink & Marsh, 2000). Ericsson (1998), Weisberg (2006), Hennessey and Amabile (2016), and Simonton (1992) studied creative people and identified at least five components that are likely to be important for creativity as listed in the table below.
Table 5.8.1. Important components for creativity
| Component | Description |
| Expertise | Creative people have studied and learned about a topic |
| Imaginative Thinking | Creative people view problems in new and different ways |
| Risk-Taking | Creative people take on new, but potentially risky approaches |
| Intrinsic Interest | Creative people take on projects for interest, not money |
| Working in Creative Environments | The most creative people are supported, aided, and challenged by other people working on similar projects |
The last aspect of the triarchic model, practical intelligence, refers primarily to intelligence that cannot be gained from books or formal learning. Practical intelligence represents a type of "street smarts" or "common sense" that is learned from life experiences. Although a number of tests have been devised to measure practical intelligence ( Wagner & Sternberg, 1985), research has not found much evidence that practical intelligence is distinct from "g" or that it is predictive of success at any particular tasks (Gottfredson, 2003). Practical intelligence may include, at least in part, certain abilities that help people perform well at specific jobs, and these abilities may not always be highly correlated with general intelligence (Sternberg et al., 1993).
Gardner's Frame of Mind
Theory of multiple intelligences: another champion of the idea of specific types of intelligences rather than one overall intelligence is the psychologist Howard Gardner (1983). Gardner argued that it would be evolutionarily functional for different people to have different talents and skills, and proposed that there are eight intelligences that can be differentiated from each other. A potential ninth intelligence, existential intelligence, still needs empirical support. Gardner investigated intelligences by focusing on children who were talented in one or more areas and adults who suffered from strokes that compromised some capacities, but not others. Gardner also noted that some evidence for multiple intelligences comes from the abilities of autistic savants, people who score low on intelligence tests overall but who nevertheless may have exceptional skills in a given domain, such as math, music, art, or in being able to recite statistics in a given sport (Treffert & Wallace, 2004). In addition to brain damage and the existence of savants, Gardner identified these 8 intelligences based on other criteria, including a set developmental history and psychometric findings. See table 5.4 for a list of Gardner's eight specific intelligences.
Table 5.8.2. Howard Gardner’s eight specific intelligences
| Intelligence | Description |
| Linguistic | The ability to speak and write well |
| Logical-mathematical | The ability to use logic and mathematical skills to solve problems |
| Spatial | The ability to think and reason about objects in three dimensions |
| Musical | The ability to perform and enjoy music |
| Kinesthetic (body) | The ability to move the body in sports, dance, or other physical activities |
| Interpersonal | The ability to understand and interact effectively with others |
| Intrapersonal | The ability to have insight into the self |
| Naturalistic | The ability to recognize, identify, and understand animals, plants, and other living things |
| Source: Adapted from Gardner, H. (1999). Intelligence Framed: Multiple Intelligences for the 21st Century. New York, NY: Basic Books. | |
The idea of multiple intelligences has been influential in the field of education, and teachers have used these ideas to try to teach differently to different students. For instance, to teach math problems to students who have particularly good kinesthetic intelligence, a teacher might encourage the students to move their bodies or hands according to the numbers. On the other hand, some have argued that these "intelligences" sometimes seem more like "abilities" or "talents" rather than real intelligence. There is no clear conclusion about how many intelligences there are. Our sense of humor, artistic skills, dramatic skills, and so forth also separate intelligences? Furthermore, and again demonstrating the underlying power of a single intelligence, the many different intelligences are, in fact, correlated and thus represent, in part, "g" (Brody, 2003).
Measuring Intelligence: Standardization and the Intelligence Quotient
The goal of most intelligence tests is to measure "g," the general intelligence factor. Good intelligence tests are reliable, meaning that they are consistent over time, and also demonstrate validity, meaning that they actually measure intelligence rather than something else. Because intelligence is such an important individual difference dimension, psychologists have invested substantial effort in creating and improving measures of intelligence, and these tests are now considered the most accurate of all psychological tests. In fact, the ability to accurately assess intelligence is one of the most important contributions of psychology to everyday public life.
Intelligence changes with age. A 3-year-old who could accurately multiply 183 by 39 would certainly be intelligent, but a 25-year-old who could not do so would be seen as unintelligent. Thus understanding intelligence requires that we know the norms or standards in a given population of people at a given age. The standardization of a test involves giving it to a large number of people at different ages and computing the average score on the test at each age level.
It is important that intelligence tests be standardized on a regular basis, because the overall level of intelligence in a population may change over time. The Flynn effect refers to the observation that scores on intelligence tests worldwide have increased substantially over the past decades (Flynn, 1999). Although the increase varies somewhat from country to country, the average increase is about 3 IQ points every ten years. There are many explanations for the Flynn effect, including better nutrition, increased access to information, and more familiarity with multiple-choice tests (Neisser, 1998). But whether people are actually getting smarter is debatable (Neisser, 1997).
Once the standardization has been accomplished, we have a picture of the average abilities of people at different ages and can calculate a person's mental age, which is the age at which a person is performing intellectually. If we compare the mental age of a person to the person's chronological age, the result is the intelligence quotient (IQ), a measure of intelligence that is adjusted for age. A simple way to calculate IQ is by using the following formula:
IQ = mental age ÷ chronological age × 100.
Thus a 10-year-old child who does as well as the average 10-year-old child has an IQ of 100 (10 ÷ 10 × 100), whereas an 8-year-old child who does as well as the average 10-year-old child would have an IQ of 125 (10 ÷ 8 × 100). Most modern intelligence tests are based on the relative position of a person's score among people of the same age, rather than on the basis of this formula, but the idea of an intelligence "ratio" or "quotient" provides a good description of the score's meaning.

Figure 5.8.1. Examples of the types of items you might see on an intelligence test.
https://assessments.lumenlearning.com/assessments/16599
Wechsler Scales
The Wechsler Adult Intelligence Scale (WAIS) is the most widely used intelligence test for adults (Watkins, Campbell, Nieberding, & Hallmark, 1995). The current version of the WAIS, the WAIS-IV, was standardized on 2,200 people ranging from 16 to 90 years of age. It consists of 15 different tasks, each designed to assess intelligence, including working memory, arithmetic ability, spatial ability, and general knowledge about the world. The WAIS-IV yields scores on four domains: verbal, perceptual, working memory, and processing speed. The reliability of the test is high (more than 0.95), and it shows substantial construct validity. The WAIS-IV is correlated highly with other IQ tests such as the Stanford-Binet, as well as with criteria of academic and life success, including college grades, measures of work performance, and occupational level. It also shows significant correlations with measures of everyday functioning among people with intellectual disabilities.
https://youtu.be/75g4d5sF3xI
Video 5.8.3. Brain vs. Bias provides an overview of the WAIS & WISC tests, standardization and validity, and IQ performance.
The Wechsler scale has also been adapted for preschool children in the form of the Wechsler primary and preschool scale of intelligence-fourth edition (WPPSI-IV) and for older children and adolescents in the form of the Wechsler intelligence scale for children-fifth edition (WISC-V).
Bias in Intelligence Testing
Intelligence tests and psychological definitions of intelligence have been heavily criticized since the 1970s for being biased in favor of Anglo-American, middle-class respondents and for being inadequate tools for measuring non-academic types of intelligence or talent. Intelligence changes with experience, and intelligence quotients or scores do not reflect that ability to change. What is considered smart varies culturally as well, and most intelligence tests do not take this variation into account. For example, in the West, being smart is associated with being quick. A person who answers a question the fastest is seen as the smartest, but in some cultures, being smart is associated with considering an idea thoroughly before giving an answer. A well- thought out, contemplative answer is the best answer.
watch it
Video 5.8.4. Watch this video to learn more about the history behind intelligence testing.
https://www.youtube.com/watch?v=7p2a9B35Xn0
Extremes of Intelligence: Intellectual Disability and Giftedness
The results of studies assessing the measurement of intelligence show that IQ is distributed in the population in the form of a Normal Distribution (or bell curve), which is the pattern of scores usually observed in a variable that clusters around its average. In a normal distribution, the bulk of the scores fall toward the middle, with many fewer scores falling at the extremes. The normal distribution of intelligence shows that on IQ tests, as well as on most other measures, the majority of people cluster around the average (in this case, where IQ = 100), and fewer are either very smart or very dull (see Figure 5.8.2). Because the standard deviation of an IQ test is about 15, this means that about 2% of people score above an IQ of 130, often considered the threshold for giftedness, and about the same percentage score below an IQ of 70, often being considered the threshold for intellectual disability.

Figure 5.8.2. Distribution of IQ Scores in the General PopulationThe normal distribution of IQ scores in the general population shows that most people have about average intelligence, while very few have extremely high or extremely low intelligence.
People with very low IQ define one end of the distribution of intelligence scores. Intellectual disability (or intellectual developmental disorder) is assessed based on cognitive capacity (IQ) and adaptive functioning. The severity of the disability is based on adaptive functioning, or how well the person handles everyday life tasks. About 1% of the United States population, most of them males, fulfill the criteria for intellectual developmental disorder, but some children who are given this diagnosis lose the classification as they get older and better learn to function in society. A particular vulnerability of people with low IQ is that they may be taken advantage of by others, and this is an important aspect of the definition of intellectual developmental disorder (Greenspan, Loughlin, & Black, 2001).
Giftedness refers to those who have an IQ of 130 or higher (Lally & Valentine-French, 2015). Having an extremely high IQ is clearly less of a problem than having an extremely low IQ, but there may also be challenges to being particularly smart. It is often assumed that schoolchildren who are labeled as "gifted" may have adjustment problems that make it more difficult for them to create social relationships. To study gifted children, Lewis Terman and his colleagues (Oden, 1968) selected about 1,500 high school students who scored in the top 1% on the Stanford-Binet and similar IQ tests (i.e., who had IQs of about 135 or higher), and tracked them for more than seven decades (the children became known as the "termites" and are still being studied today). This study found that these students were not unhealthy or poorly adjusted, but rather were above average in physical health and were taller and heavier than individuals in the general population. The students also had above-average social relationships and were less likely to divorce than the average person (Seagoe, 1975).
Terman's study also found that many of these students went on to achieve high levels of education and entered prestigious professions, including medicine, law, and science. Of the sample, 7% earned doctoral degrees, 4% earned medical degrees, and 6% earned law degrees. These numbers are all considerably higher than what would have been expected from a more general population. Another study of young adolescents who had even higher IQs found that these students ended up attending graduate school at a rate more than 50 times higher than that in the general population (Lubinski & Benbow, 2006).
As you might expect based on our discussion of intelligence, kids who are gifted have higher scores on general intelligence "g," but there are also different types of giftedness. Some children are particularly good at math or science, some at automobile repair or carpentry, some at music or art, some at sports or leadership, and so on. There is a lively debate among scholars about whether it is appropriate or beneficial to label some children as "gifted and talented" in school and to provide them with accelerated special classes and other programs that are not available to everyone. Although doing so may help the gifted kids (Colangelo & Assouline, 2009), it also may isolate them from their peers and make such provisions unavailable to those who are not classified as "gifted."
